



ACE-SUPPORTED RESEARCH: Does the ACE Integrated Fitness Training® Model Really Work? (Year 2 Study)
Certified™: July 2022

What You Need to Know
This is the second report on an ongoing three-year study examining the effectiveness of exercise programming based on the ACE Integrated Fitness Training® Model. The results of this study provide additional support to the findings of previous ACE-supported research on the Model—namely, that the personalized approach optimizes training responsiveness and positively impacts cardiorespiratory fitness, muscular fitness and cardiometabolic health.

Since first introducing the ACE Integrated Fitness Training (ACE IFT®) Model more than a decade ago, ACE has been supporting research to investigate its effectiveness in real-world settings, focusing on various elements related to the Model, including training responsiveness, exercising in a community setting, exercise for older adults and behavior and lifestyle change.
In 2021, we presented the results of Year 1 of a multi-year, multi-site study examining the effectiveness of personalized exercise programming using the ACE IFT Model at eliciting favorable comprehensive training responsiveness (i.e., cardiorespiratory fitness + muscular fitness + cardiometabolic health).
Here, we present the findings of Year 2 of this three-year investigation. Like the Year 1 study, this research was conducted by Lance Dalleck, PhD, and his team of researchers in the High Altitude Exercise Physiology Program at Western Colorado University. At the conclusion of this project, the research will provide a robust body of data from more than 100 participants.
The Study
Twenty-seven nonsmoking men and women ranging in age from 21 to 65 years old were recruited to participate in a 13-week study. All were physically inactive, which is defined as not having participated in at least 30 minutes of moderate-intensity physical activity on at least three days of the week for at least three months, and all were asked to continue their current dietary habits and to not perform additional exercise beyond that required for the research. None of the participants had evidence of cardiovascular, pulmonary and/or metabolic disease, as determined by the completion of a medical history questionnaire.
The participants underwent two days of baseline measurements prior to the beginning of the study. The following variables were measured:
- Resting heart rate
- Resting blood pressure
- Anthropometric measurements: Height, weight, percent body fat, and waist and hip circumferences
- Fasting blood lipids
- Fasting blood glucose
- Assessments for muscular strength: Five-repetition maximum (5-RM) for the bench press and leg press exercises
- Maximal exercise testing: Maximal oxygen consumption (VO2max) and maximal heart rate [note that heart-rate reserve (HRR) was calculated for each participant by subtracting resting heart rate from maximal heart rate]
- First and second ventilatory thresholds (VT1 and VT2)
After completing the baseline assessments, the participants were randomized into three groups:
- ACE IFT Model group
- Standardized training group
- Control group
Cardiorespiratory Training
The cardiorespiratory exercise was performed on various modalities: arm, cycle and rowing ergometers; elliptical crosstrainers; and treadmills. The standardized training group worked at an intensity based on a percentage of their HRR, while those in the ACE IFT Model group received programming based on their ventilatory thresholds. For both groups, a target heart rate was determined to coincide with either the HRR or ventilatory thresholds to establish a specific intensity for each exercise session.
The cardiorespiratory training programs progressed for both groups over the course of the 13 weeks. Frequency remained consistent for both exercise groups, at three workouts per week throughout the study.
For the standardized training group, cardiorespiratory exercise began in week 1 at 40 to 45% of HRR for 25 minutes per day. The duration of each training session was extended by 5 minutes each week until weeks 5 and 6, when intensity increased to 50 to 55% HRR for 45 minutes per day. Then, in weeks 7 and 8, duration increased to 50 minutes per day. For the final five weeks of the study, this group exercised at 60 to 65% HRR for 50 minutes per day.
For the ACE IFT Model group, cardiorespiratory exercise began at a heart rate below VT1 for 25 minutes per day. As with the standardized training group, the duration of training sessions was extended by 5 minutes per week until weeks 5 and 6, when intensity increased to a heart rate equal to or greater than VT1 but below VT2. Then, in weeks 7 and 8, duration increased to 50 minutes per day. For the final five weeks of the study, this group exercised at an intensity equal to or greater than VT2 for 50 minutes per day.
Muscular Training
Muscular training was introduced during week 4 and continued to be performed three days per week through week 13.
For the standardized training group, the program consisted of the following single- and multijoint exercises performed on machines:
- Bench press
- Shoulder press
- Lat pull-down
- Seated row
- Biceps curl
- Triceps push-down
- Seated leg press
- Seated leg extension
- Prone leg curl
- Seated back extension/flexion
Two sets of 12 repetitions were completed for each exercise. Resistance was progressed every two weeks by approximately 3 to 5% of the total weight lifted for the upper body and approximately 6 to 10% for lower-body exercises. A session rating of perceived exertion (RPE) of 5 to 6 on the 0-to-10 scale was maintained across the training program.
For the ACE IFT Model group, muscular training consisted of multijoint/multiplanar exercises using both free weights and machines. The machines allowed for free motion during the exercises, meaning that range of motion was not limited to a specific arc. The following exercises were performed:
- Stability ball circuit (glute bridges, crunches, Russian twists, planks)
- Lunge matrix
- Kneeling/standing wood chops
- Kneeling/standing hay balers
- Dumbbell squat to 90-degree knee bend
- Standing one-arm cable row
- Step-ups with dumbbell onto a 6-inch (15-cm) step
- Modified (assisted) pull-ups
- Dumbbell bench press
Two sets of 12 repetitions were completed for each exercise. The intensity of weighted exercises started at 50% of 5-RM and was progressed by 5% of 5-RM increments every two weeks. For exercises that did not include a weighted resistance (e.g., stability ball circuit), the number of repetitions was increased by approximately 5 to 10% to maintain an RPE rating of 5 to 6 on the 0-to-10 scale.
Figure 1 provides a flow chart of the experimental procedures and exercise programs for all three groups.

The Results
At the end of the 13-week program, participants from all three groups repeated the measurements taken at the outset. Note that the data and analyses presented here are for Year 2 participants only. Also, it is important to note that the three groups did not differ in physical or physiological characteristics prior to the study.
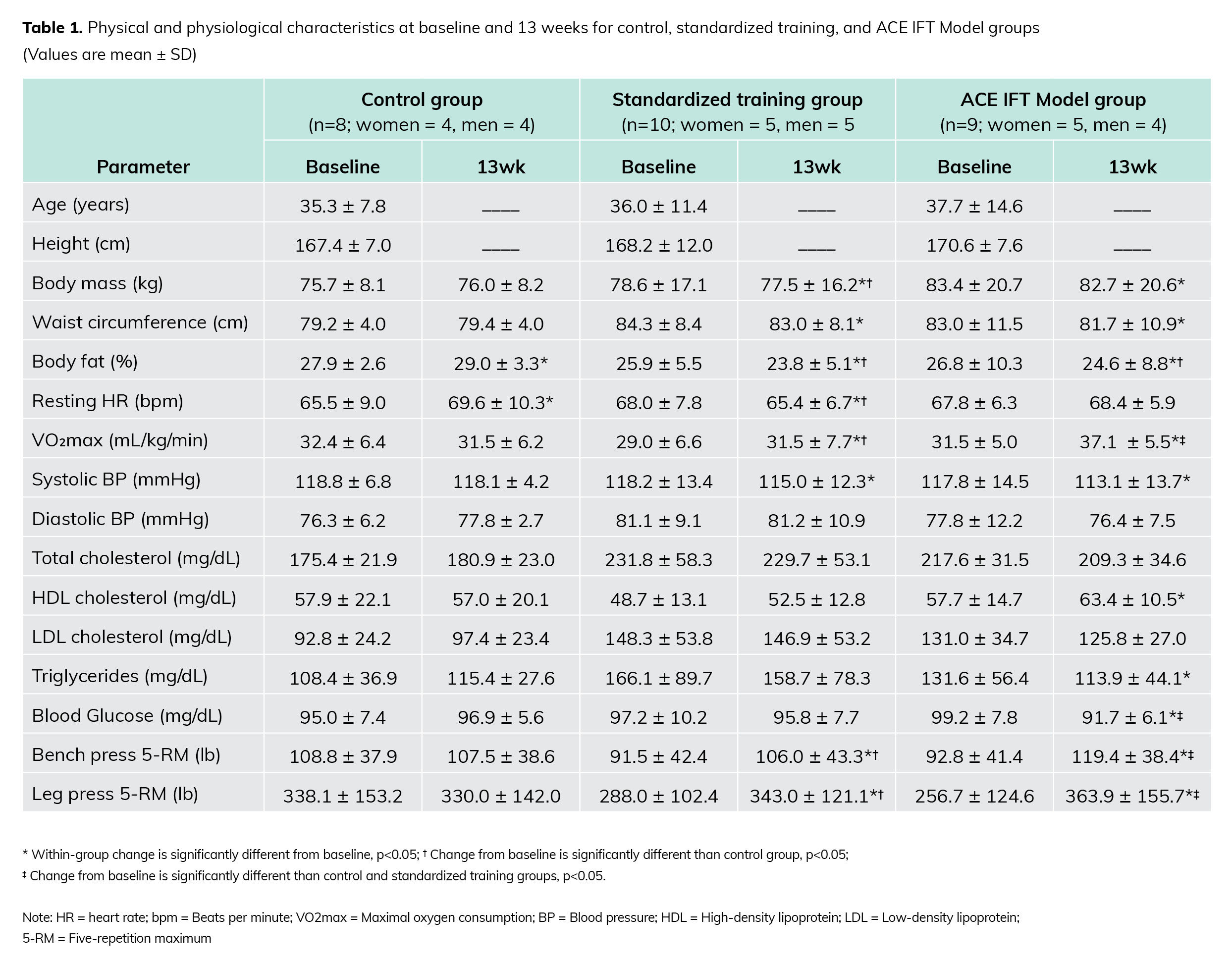
Here are the key findings, as presented in Table 1:
- After 13 weeks, the following measures were statistically significantly more desirable in the standardized training group as compared to the control group: body mass, body-fat percentage, resting heart rate, VO2max, bench press 5-RM and leg press 5-RM.
- The change in body-fat percentage was statistically significantly more desirable in the ACE IFT Model group relative to the control group.
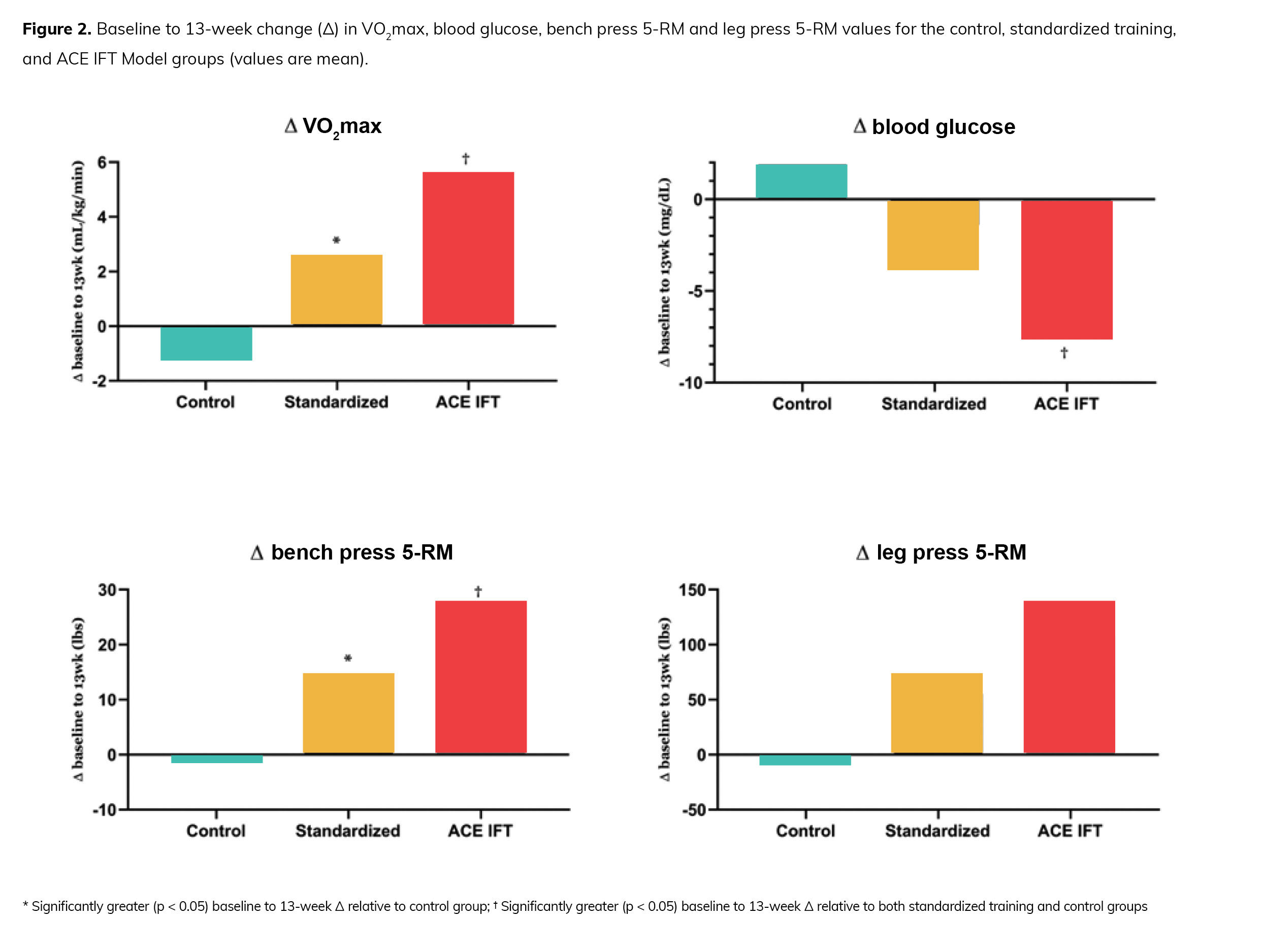
- The changes in VO2max, blood glucose, bench press 5-RM and leg press 5-RM were statistically significantly more favorable in the ACE IFT Model group when compared to both the standardized training group and the control group (Figure 2).
Highlighting the Importance of Muscular Fitness
Over the past decade, low muscular fitness has garnered considerable attention as an independent and powerful predictor of chronic disease risk and premature mortality. Indeed, it has been reported that increased muscular fitness is associated with a reduced risk of all-cause mortality. Additionally, various muscular fitness parameters (e.g., strength, endurance and power) have been found to be associated with common cardiometabolic risk factors, including body mass index, waist circumference, blood lipids and blood pressure. It also has been demonstrated that that there is a strong association between muscular strength and mortality from all causes in various clinical populations, including those with cardiovascular disease, cancer and arthritis. More recently, elevated levels of both upper- and lower-body muscular strength have been linked to lower risk of mortality. Finally, it has been shown that a moderate level of muscular strength is associated with a 32% lower risk of developing type 2 diabetes.
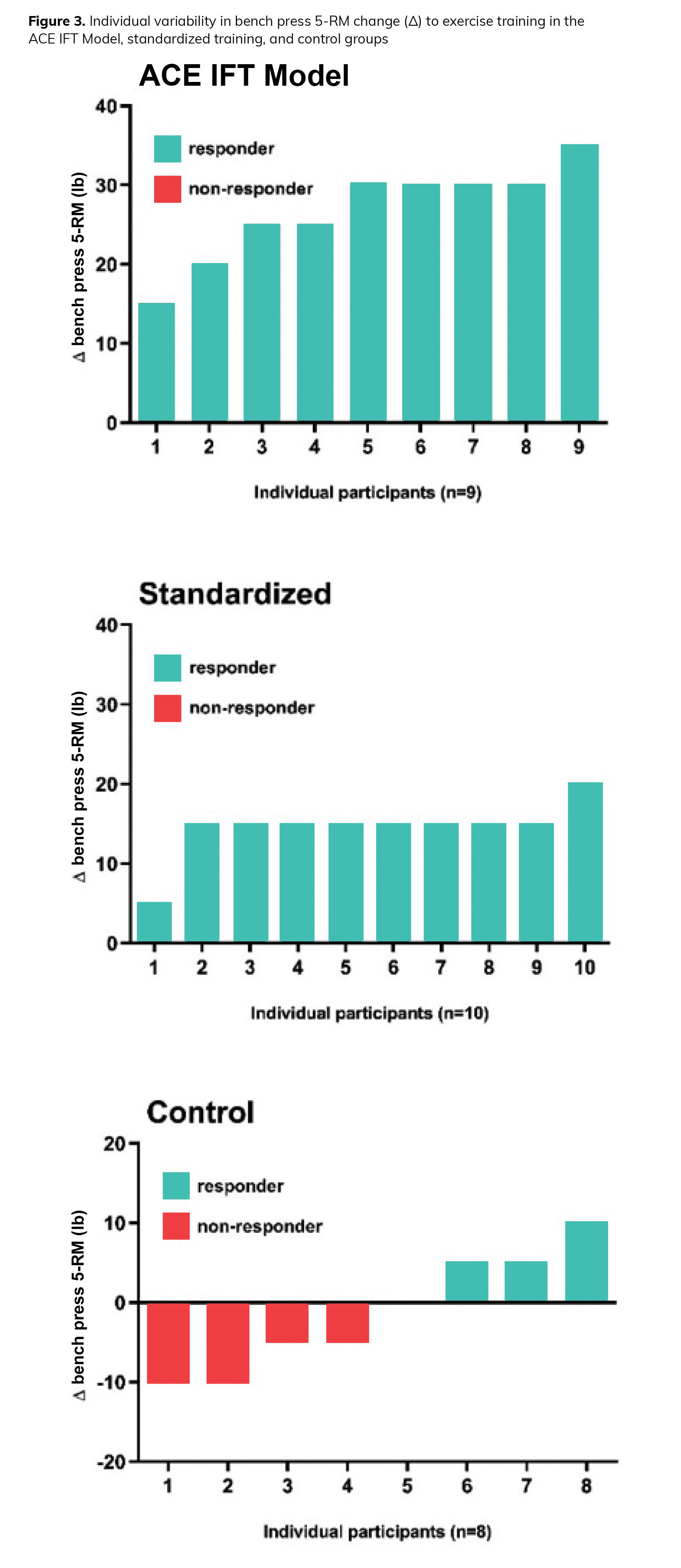
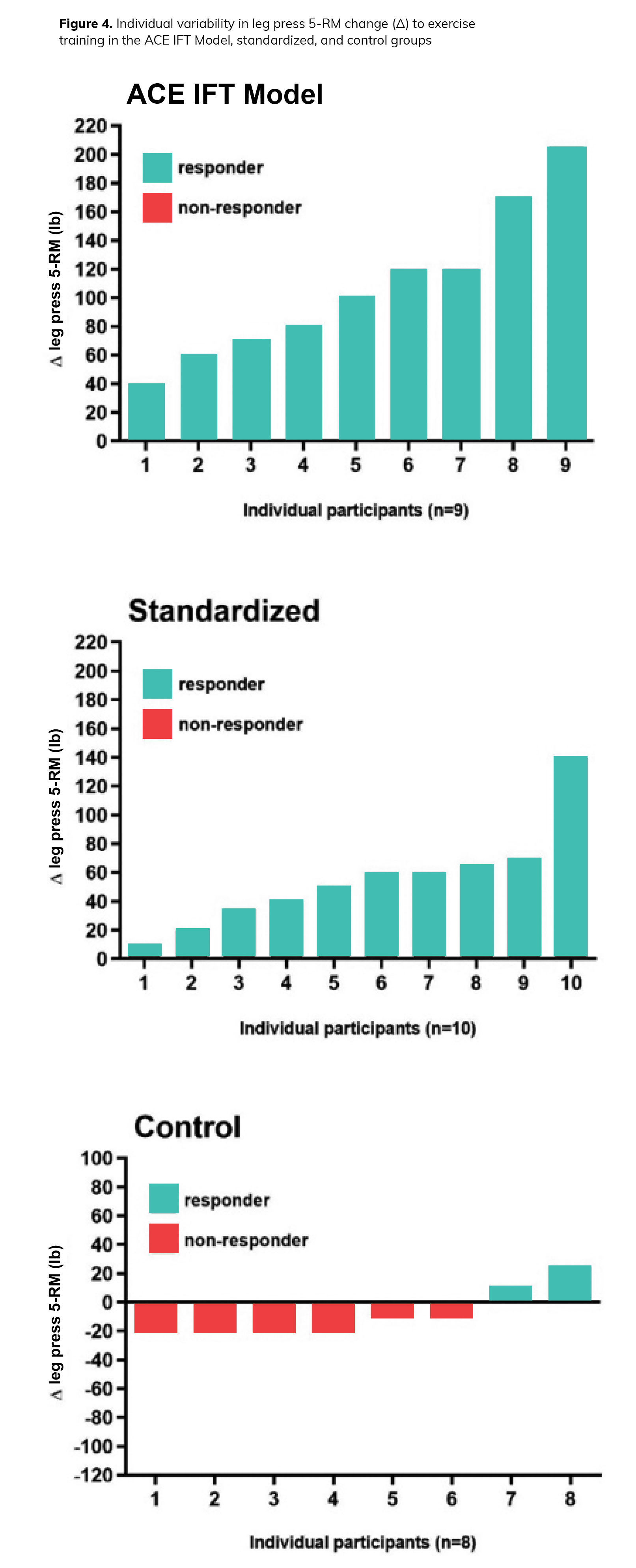
“Taken together,” explains Dr. Dalleck, “this body of scientific literature highlights the critical long-term role of muscular fitness for overall client health.” In Year 2 of this ongoing study, it was demonstrated that a personalized exercise program using the ACE IFT Model enhanced training efficacy and limited training unresponsiveness with respect to both cardiorespiratory fitness (i.e., VO2max) and muscular fitness (i.e., 5-RM bench press and leg press). In particular, the muscular fitness findings are novel. As presented in Figures 3 and 4, the individual changes in 5-RM bench press and 5-RM leg press are consistently twofold greater across all ACE IFT Model group participants when compared to their standardized training and control group counterparts. “These muscular fitness responsiveness findings highlight the importance of personalizing the exercise program,” says Dr. Dalleck, “which is accomplished best with the ACE IFT Model.”
In Conclusion
In the present study, a personalized exercise program using the ACE IFT Model, which combined cardiorespiratory training in conjunction with muscular training elicited significantly greater improvements in VO2max, muscular fitness and various cardiometabolic outcomes (e.g., fasting blood glucose values) combined with diminished inter-individual variation in training responses when compared to standardized exercise training and a non-exercise control group. These findings continue to be encouraging and provide insightful data on the effectiveness of personalized exercise programming.
As Dr. Dalleck explains: “When we personalize the exercise program, for both cardiorespiratory and muscular training, versus a more standardized approach, we’re almost always seeing VO2max and muscular strength improve, whereas with a more one-size-fits-all or standardized approach, we’re diminishing training responsiveness by about a third. This really underpins why the ACE IFT Model is so successful.”
Expand Your Knowledge
 |
Exercise Programming Toolkit – Course BundleThe ACE Integrated Fitness Training® Model Exercise Programming Toolkit course bundle explores the different components of the ACE IFT® Model, including the ACE Mover MethodTM, to help you develop safe and effective exercise plans. By gaining an understanding of how to move through the phases of the ACE IFT Model, you will be able to effectively educate clients and gain their trust, keeping them safe as they move toward their goals. |
 |
Essential Toolkit for Exercise Professionals – Course BundleThe Essential Toolkit for Exercise Professionals course bundle, you will discover key skills to help your clients achieve their fitness goals. From behavior-change strategies, nutrition coaching, strength training and more, you will build the foundation for success as an exercise professional. |
 |
Strategies for Enhancing Program Design – Course BundleWhen designing an exercise program for clients, there are many ways to create safe and effective training plans. The Strategies for Enhancing Program Design – Course Bundle will elevate your exercise programs by showing you how to integrate agility training, HIIT and the ACE Integrated Fitness (ACE IFT) Model. |


More Articles
- Certified™: July 2022
Sandbag Training 2.0: An ACE Integrated Fitness Training Model® Workout
Health and Fitness Expert
- Certified™: July 2022
Goal Setting and the Ethics of Steering a Client Toward Different Goals
Contributor
- Certified™: July 2022
How to Help Clients Manage the Common Risk Factors for Diabetes and Heart Disease
Health and Fitness Expert