



Fish Oil Showdown: Anti-inflammatory Effects of EPA vs. DHA
ProSource™: September 2016

Chronic inflammation has been identified as a potential link between obesity and cardiovascular diseases. In people who have obesity, fat cells release greater amounts of inflammatory and signaling molecules (adipokines) that induce insulin resistance, blood vessel dysfunction, and systemic inflammation, all of which increase the likelihood that an artery may become damaged. Once damaged, the artery will express proteins that attract white blood (immune) cells to the location to help with repair and recovery. These immune cells also begin secreting chemicals (cytokines) that signal more immune cells to come to their location.
At this point, the damage should resolve and everything would be fantastic, if that actually happened. However, the chronic inflammation and dyslipidemia associated with obesity continually damages the arteries, never allowing them to fully repair. Accordingly, immune cells (macrophages, especially) continue to accumulate. While all this is going on, LDL particles float through the blood trying to do their job. If a lot of LDL particles are present, then there is an increased chance that some of them become trapped in the damaged artery and become oxidized. If that happens, the macrophages will eat them, thinking they’re doing the body a favor. This engulfment occurs over and over again until the macrophage is filled with lipids and becomes a “foam” cell. Foam cells cannot function properly and ultimately accumulate to form part of the plaque seen in atherosclerosis.
There is a growing body of literature suggesting that the omega-3 fatty acids EPA and DHA have the potential to reduce the inflammatory state associated with obesity. EPA and DHA serve as the precursor molecules from which anti-inflammatory compounds (resolvins, protectins and maresins) are synthesized. A recent meta-analysis of 68 randomized controlled trials (RCTs) and 4601 individuals showed that EPA and DHA supplementation significantly reduced several inflammatory molecules: tumor necrosis factor alpha (TNFα), C-reactive protein (CRP, described further in Figure 1), and interleukin-6 (IL-6).
Figure 1
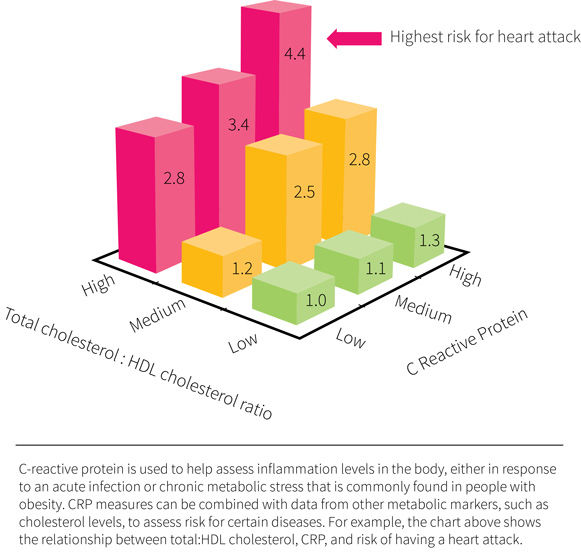
However, this meta-analysis also revealed notable research gaps. For instance, nearly all the included studies used either a combination of EPA and DHA or used only one of the fatty acids in isolation. It therefore remains unknown whether EPA and DHA have similar or different effects on inflammatory markers. The current study was designed specifically to fill this knowledge gap and determine how EPA and DHA compare when it comes to reducing inflammation.
Obesity is associated with chronic inflammation that plays an important role in cardiovascular diseases. Current evidence suggests that EPA and DHA supplementation is an effective option for reducing inflammation, but whether one is more effective than the other remains unknown. The current study was designed to pit EPA against DHA and find out whether one could be considered more anti-inflammatory than the other.
Who and What Was Studied?
This was a double-blind, randomized, placebo-controlled crossover study in which participants supplemented with 2.7 grams per day of EPA, 2.7 grams of DHA, or three grams of corn oil (control) for about 10 weeks each. The supplements were supplied as three identical one-gram capsules. The EPA and DHA were in the form of re-esterified triglycerides from fish oil (meaning the EPA and DHA fatty acids were separated from the glycerol backbone of the triglycerides present in fish oil and then put back together so that all three of the fatty acids making up each triglyceride were either EPA or DHA). Each phase was separated by a nine-week washout period.
A total of 154 men and women began the intervention, but only 123 completed it. This approximately 20 percent dropout rate was substantial, but considered acceptable for a trial this long (spanning roughly one year). All participants considered for this trial had abdominal obesity (waist circumference greater than 80 centimeters for women and greater than 94 centimeters for men) in combination with a plasma CRP value of greater than one but less than 10, but were otherwise healthy. People with a history of cardiovascular diseases, taking medications known to affect inflammation, or using fish oil supplements within two months of beginning the study were excluded.
During each study phase, the participants were instructed to maintain their bodyweight and exclude fatty fish, fish oil supplements, flax products, walnuts, and omega-3 enriched products from their diets. Compliance to supplementation was assessed by pill counting, and a subsample of thirty participants also had plasma phospholipid concentrations of EPA and DHA measured. Diets were monitored for change through a food frequency questionnaire.
Before and after each intervention phase, assessments were made for body composition (DXA), inflammatory markers (CRP, IL-6, TNFα, IL-18, and adiponectin), and blood lipids. All variables except for TNFα and IL-18 were measured twice on consecutive days to reduce variation and increase statistical power. Plasma CRP served as the primary outcome because it is considered a key variable for the assessment of inflammatory status. Other variables were secondary outcomes.
Men and women with abdominal obesity and low-grade inflammation consumed 2.7 grams of EPA, 2.7 grams of DHA, or three grams of corn oil for 10 weeks each in a double-blind, randomized, placebo-controlled crossover study. Inflammatory molecules, blood lipids, and body composition were assessed before and after each phase.
What Were the Findings?
The study results are shown in Figure 2. Compared to the control, only DHA significantly reduced CRP (-7.9 percent), but this reduction was not significantly different from EPA (-1.7 percent vs control). Additionally, both EPA and DHA significantly reduced IL-6 (-13.4 percent and -12 percent, respectively), but only DHA significantly reduced IL-18 (-7 percent) and TNFα (-14.8 percent) and significantly increased adiponectin (+3.1 percent) when compared to control. The reduction in IL-18 and increase in adiponectin were significantly greater with DHA than EPA. There were no significant differences between men and women for changes in inflammatory markers.
Figure 2
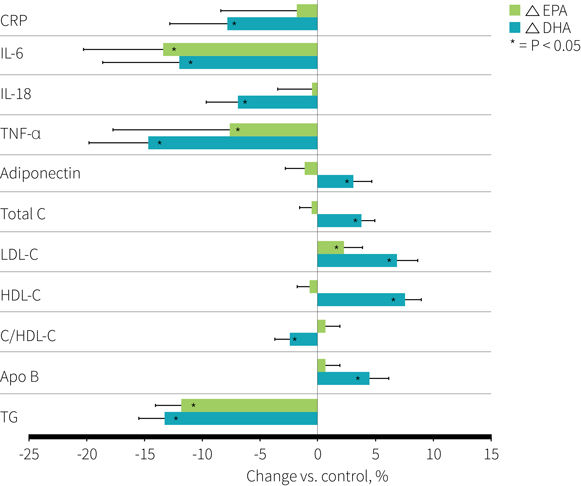
Compared to the control, both EPA and DHA significantly increased LDL-c (+2.2 and +6.9 percent) and reduced triglycerides (-11.9 and -13.3 percent), but only DHA significantly increased total cholesterol (+3.8 percent), HDL-c (+7.6 percent), and apoB (+4.5 percent) and significantly reduced the total cholesterol to HDL-c ratio (-2.5 percent). Additionally, the increases in total cholesterol, LDL-c, HDL-c and the decreases in triglycerides and the total cholesterol to HDL-c ratio were significantly greater with DHA than with EPA.
The only significant difference between men and women in blood lipid responses was that DHA supplementation increased LDL-c more than EPA in men (12.5 percent vs. 5.1 percent) but not women (4.4 percent vs. 3.0 percent). There were no significant differences between EPA, DHA, and control for changes in bodyweight or body composition.
Compliance to supplementation was greater than 96 percent for all groups, and as expected the phospholipid fatty acid profile tracked well with each supplementation phase. The control led to significantly greater concentrations of total omega-6 fatty acids, linoleic acid, and arachidonic acid compared to EPA and DHA. Conversely, EPA and DHA significantly increased total omega-3 concentrations to a similar extent compared to the control, with EPA significantly increasing EPA but not DHA concentrations and DHA significantly increasing DHA but not EPA concentrations.
Compared to corn oil, DHA supplementation affected numerous inflammatory markers and blood lipids, including a significant reduction of CRP, whereas EPA was more limited in its effects. Additionally, DHA was more effective than EPA in changing blood lipids and some inflammatory markers.
What Does the Study Really Tell Us?
This study suggests that the beneficial effects of fish oil supplementation on markers of inflammation and blood lipids may be owed primarily to DHA rather than EPA, at least among abdominally obese men and women with low-grade systemic inflammation.
This is the largest randomized crossover trial to date that provides a comparison of the effects of EPA and DHA on inflammatory markers. However, a priori analysis determined that 150 individuals would be needed to detect a minimal difference of 10 percent in CRP concentrations between any two groups. Yet, dropouts reduced the sample size to 123 participants, and the largest difference observed was only 8 percent between DHA and the control. The lower sample size and magnitude of change may explain why the average reduction in CRP failed to reach significance between EPA and DHA despite DHA leading to a nearly four-fold greater reduction than EPA. However, using an intent-to-treat analysis that imputed the missing data from the dropouts didn’t change the results. Also, the study did detect a significant difference between DHA and corn oil, so the study wasn’t grossly underpowered.
It’s important to remember that the current study investigated CRP as its primary endpoint, meaning that the outcomes for other inflammatory markers and blood lipids weren’t necessarily sufficiently powered (and mostly likely weren’t) to detect significant differences between groups. Therefore, while this study does support the notion that DHA is more effective than EPA at modulating a handful of inflammatory markers and blood lipids, future head-to-head studies are needed to confirm these findings. Notably, a meta-analysis of six studies comparing the effect of EPA to DHA on blood lipids did confirm the current study’s findings that DHA raises LDL-c and HDL-c and reduces triglycerides to a greater extent than EPA.
The question remains whether a combination of EPA and DHA would be more effective than either in isolation. A fourth group consuming both EPA and DHA in the current study could have answered this question. Also, the use of corn oil as a control may have exaggerated the effects of EPA and DHA on some study outcomes. Compared to baseline values, corn oil was shown to significantly reduce total and LDL-cholesterol values, but no other outcome variables, which may explain why these blood lipids were elevated with EPA and DHA supplementation. Finally, whether the results would be similar or different among people without abdominal obesity or low-grade inflammation remains unknown. At least one study has suggested that consuming 1400 milligrams per day of EPA plus DHA has no significant effect on serum CRP or IL-6 concentrations of healthy adults (although they were somewhat similar to the current study in that these individuals were, on average, overweight and some had a CRP value above one).
DHA may be more effective than EPA at reducing low-grade inflammation and improving blood lipids among individuals with abdominal obesity and systemic low-grade inflammation. However, this study was designed primarily to examine differences in CRP, limiting our ability to form conclusions about other inflammatory biomarkers and warranting more research to verify the findings.
The Big Picture
A recurring ERD topic is the concept of reductionism, or the idea that the whole is nothing more than the sum of its individual components. As discussed in ERD #2, reductionism has led to many meaningful discoveries in Western science and medicine. However, its benefits are far more limited when it comes to nutrition, owed in no small part to the fact that reductionism doesn’t reflect the way we actually eat or how foods are metabolized in the body.
An example of the above was shown in ERD #8, where two groups of participants consumed diets identical in calories and macronutrients, with the only difference being the foods supplying them. On the one hand, there was a group chowing down on “paleo” foods like lean meats, eggs, and starchy tubers, while on the other hand was a group obtaining their carbohydrates primarily from cereal grains and legumes. The paleo diet group showed significantly greater improvements for insulin sensitivity, glycemic control, and blood lipid values.
With fish oil being one of the most widely used supplements, it is important not to start over-emphasizing DHA due to this one study. With so many health-related biomarkers not tested in the study at hand, it is premature to conclude that DHA is more important than EPA. For instance, some evidence suggests that EPA, but not DHA, improves symptoms of depression. This may be due to one of the many genes shown to have their expression modified by EPA but not DHA supplementation. EPA and DHA exist together in nature, and while their ratios may differ depending on the animal, there may be benefits to consuming both that are not obtainable when consuming either in isolation.
Studies like this should not be analyzed through the frame of a reductionist mindset. EPA and DHA exist together in nature and there are factors that may only respond to combined EPA and DHA consumption.
Frequently Asked Questions
Does alpha-linolenic acid have anti-inflammatory effects?
A recent meta-analysis of 20 randomized controlled trials looking at the effect of alpha-linolenic acid (ALA) on plasma CRP concentrations reported that, overall, flaxseed or ALA supplementation did not have a significant effect. However, subgroup analysis suggested that a significant reduction in CRP could be obtained in participants with a BMI greater than 30 and possibly when baseline CRP values were greater than 10 mg/mL. Even so, publication bias was present, warranting caution with these results.
Does the type of supplement matter? Triglycerides vs. ethyl esters vs. phospholipid-bound?
EPA and DHA supplements come in three flavors: bound to phospholipids, bound to triglycerides, and as ethyl esters. Around 95 percent of dietary fat and most of the storage fat within the body are triglycerides. However, phospholipids are the primary component of cell membranes, so it is easy to see why some may argue that this form is superior for EPA and DHA supplementation. In contrast to these naturally occurring forms of delivery, ethyl esters are synthetically created by reacting EPA and DHA with alcohol so as to selectively concentrate the fatty acids and allow for more concentrated fish oil supplements.
At least one study has compared all three forms for their ability to modulate red blood cell membrane concentrations of EPA and DHA. Sixty-six healthy adults supplemented with 1.3 grams of EPA plus DHA for four weeks, supplied as krill oil (40 percent phospholipids), a fish oil triglyceride supplement (the most common form on the market), and an EPA plus DHA ethyl ester.
After the four-week supplementation period, total red blood cell concentrations of EPA plus DHA were not significantly different between the three groups, although both krill oil and the triglyceride fish oil led to about 14 percent greater concentrations than the ethyl ester. However, krill oil usually sells for a premium in comparison to fish oil triglycerides. So, it may be more financially prudent to buy regular fish oil.
What Should I Know?
The study under review is the largest randomized, crossover, placebo-controlled study to pit EPA and DHA against one another with regard to their effects on inflammation and blood lipids.
DHA appears to have a more pronounced effect than EPA for lowering C-reactive protein and several other inflammatory markers. DHA also appears to have a more favorable effect on blood lipids, such as a reduction in triglycerides and the total cholesterol to HDL-c ratio (although LDL-c was notably increased, which warrants further research). However, many of the differences between DHA and EPA were not significant and the magnitude of difference between EPA and DHA was not huge. Additionally, many variables were not assessed in the current study and some research shows EPA to have unique effects not observed with DHA supplementation. Therefore, it is important to avoid a reductionist mindset and remember that EPA and DHA come packaged together in nature, and concentrating on one of them may not be necessary for most people.
Reproduced with permission from Examine.com. All rights reserved.

More Articles
- ProSource™: September 2016
The Art of Intelligently Sequencing Yoga Classes
Health and Fitness Expert
- ProSource™: September 2016
Effective Strategies for Exercise Cueing
Health and Fitness Expert
- ProSource™: September 2016
Coaching Behavior Change: How to Plan For and Address Relapses
Health and Fitness Expert