In an effort to help you more efficiently earn continuing education credits while you explore
CERTIFIED™, you can now take the quiz as you read. Get the latest, science-based information
while you earn 0.2 CECs.
As a health and exercise professional, you routinely cue clients to stretch, warm up and improve range of motion (ROM), but ROM alone shouldn’t be the goal. A client may demonstrate adequate passive flexibility during an assessment yet still struggle to squat, rotate, reach overhead or control a single-leg stance during functional tasks. That disconnect reflects the difference between flexibility and mobility. Flexibility describes the available range at a joint, usually influenced by the extensibility of muscle and connective tissue. Mobility describes usable range, which is the ability to actively move and control a joint through that ROM with strength, coordination and balance. In this article from Pete McCall, MS, fitness educator and creator of Strength Training for Longevity with Pete McCall, you'll learn how mobility and flexibility differ, why this matters for assessment and program design, and how to apply both concepts to help clients move more effectively.
This distinction has important implications for exercise programming. A client who lacks tissue extensibility may benefit from targeted stretching strategies. A client who demonstrates passive range but cannot control that range during movement needs a different approach—one that improves neuromuscular coordination and reinforces efficient movement patterns. For clients, the benefits can include better movement quality, improved exercise technique, greater tolerance to training and more confidence during everyday activities. For professionals, understanding the difference leads to more precise assessments and more effective exercise selection (Table 1). Flexibility contributes to mobility, but mobility is what determines whether available range can be used effectively.
Table 1. Characteristics of Flexibility and Mobility
Characteristic
Flexibility
Mobility
Primary emphasis
Available or passive ROM; tissue length and stretch tolerance
Usable ROM; active control through available range
What it requires
Extensibility of muscle and connective tissue
Flexibility plus strength, coordination, balance and motor control
Common methods
Static stretching, prolonged holds and passive positioning
Dynamic drills, controlled joint motion and movement-based patterns
Best programming uses
Cool-downs, recovery work and stretching for restricted tissues
Warm-ups, movement preparation, technique work and active recovery
Flexibility reflects passive capacity. Mobility reflects active control of that capacity during real movement.
Flexibility Measures Capacity; Mobility Measures Control
Flexibility is most often discussed as the ability of a muscle or muscle group to lengthen. In practice, this is usually observed when a joint moves passively or when a stretch is held long enough for tissue tension to decrease. Static stretching, partner-assisted stretching and other passive methods can increase tolerance to stretch and, over time, may improve passive ROM. This can be useful when short or stiff tissues limit motion or when reducing post-exercise tension is the primary goal.
A closely related term is extensibility, which refers to the mechanical ability of muscle and connective tissue to lengthen and shorten as joint motion occurs. Extensibility matters because tissues must allow movement to happen, but it still does not fully describe whether a client can actively control that movement. That is where mobility becomes the more useful programming concept.
Mobility is the ability to actively produce and control movement through available ROM. It depends not only on tissue length, but also on muscular strength, timing, coordination, balance and the quality of sensory input reaching the nervous system. As one set of muscles contracts to move a joint, the muscles on the opposite side of the joint must lengthen to allow that motion. Sensory receptors in muscles, fascia, joint capsules and ligaments continually relay information about tension, position and speed back to the central nervous system, which then adjusts force production and joint position in real time. In other words, mobility is range of motion the body can organize, stabilize and use.
This distinction explains why a client can look “flexible” and still move poorly. For example, a client may have enough passive hip flexion when lying on a table yet struggle to control hip motion during a squat or lunge. Another client may reach overhead when assisted but compensate with lumbar extension when trying to press a weight. In both cases, the missing piece is active control, not simply more length. Likewise, improving flexibility without improving strength and coordination can create range the client cannot own, which may increase instability at a joint rather than improve movement quality.
For programming purposes, flexibility and mobility should be viewed as complementary but not interchangeable. Flexibility provides the potential for movement. Mobility determines whether that potential can be expressed during real tasks such as walking, squatting, pushing, rotating or changing direction. This is why pre-exercise preparation should rarely focus on passive stretching alone. Before movement, the goal is to prepare the nervous system and the muscles to produce force throughout useful ROM. Dynamic mobility drills, controlled articular rotations, body-weight movement patterns and low-load multiplanar exercises are often better suited to that purpose because they combine motion with activation and control.
Why Mobility Is Foundational for Moving Well
The human body does not move one muscle at a time. Walking, getting up from the floor, lifting groceries, climbing stairs, swinging a golf club and performing a loaded hinge all require multiple joints and tissues to work together in three dimensions. Because of that, mobility should not be viewed as separate from movement skill. Rather, it is one of the foundations of movement skill.
When a program emphasizes only linear, isolated movements, clients may develop strength in specific patterns without learning how to coordinate motion through the feet and ankles, hips, thoracic spine, shoulders and trunk. Mobility training restores that integrated quality. Slow, deliberate multidirectional drills teach the body how to share motion across segments. They also improve a client’s awareness of where the body is in space—an essential component of balance, technique and injury prevention.
This is one reason movement-based training environments often prioritize mobility before heavy loading. Athletes do not improve performance simply by becoming more “bendy.” They improve by being able to access joint motion while maintaining alignment, stiffness where needed and sequencing from one segment to the next. The same principle applies to the general population. A client who can control hip extension and thoracic rotation during gait will usually move more efficiently than a client with similar passive ROM but poor timing and coordination.
Mobility also helps preserve what has been described as a client’s envelope of function (EOF); this term was introduced by Dr. Scott Dye, an orthopedic surgeon, in 1996 to describe the amount of movement a person can perform comfortably and confidently in daily life. Movements like deep squatting to pick up a child, rotating to back a car out of a driveway, reaching into an overhead cabinet, getting off the floor or stepping over obstacles all depend on active ROM. When mobility declines, ordinary tasks become higher-effort tasks. When it improves, activities of daily living remain well below maximum capacity—meaning that the person is capable of doing much more than their daily activities require—which is especially important for long-term independence.
At the tissue level, movement itself supports joint health. Articular cartilage depends on movement and changes in pressure for nutrient exchange, and regular motion helps circulate synovial fluid through the joint. Repeated movement through safe ROM also exposes the nervous system to controlled variations in load and position, which can sharpen coordination. From a practical standpoint, mobility work is one of the most efficient ways to prepare clients to move well, train well and recover well—without requiring high impact or high fatigue.
Mobility is also context specific. The amount of range needed for a powerlifter’s squat, a runner’s stride, an overhead press and getting down to the floor with a grandchild are not identical. That’s why it’s not necessary to chase maximal ROM at every joint. Instead, focus on helping clients develop enough motion to meet the demands of a given task while maintaining alignment and control. This keeps programming centered on function rather than appearance. A deep passive stretch may look impressive, but if it does not improve the client’s ability to squat, rotate, reach or change levels safely, it has limited training value.
Mobility is especially valuable for clients whose routines expose them to repetitive or restricted movement options. Long hours of sitting can reduce hip extension and thoracic rotation. Running, cycling and many machine-based resistance exercises are dominated by repetitive, mostly linear patterns. Multiplanar mobility work restores variability by exposing the body to flexion, extension, rotation and lateral movement that may be missing elsewhere in the client’s week. That variability helps distribute stress across tissues, reinforces healthier movement options and can make the rest of the exercise program more effective.
A Joint-by-Joint Perspective on Mobility
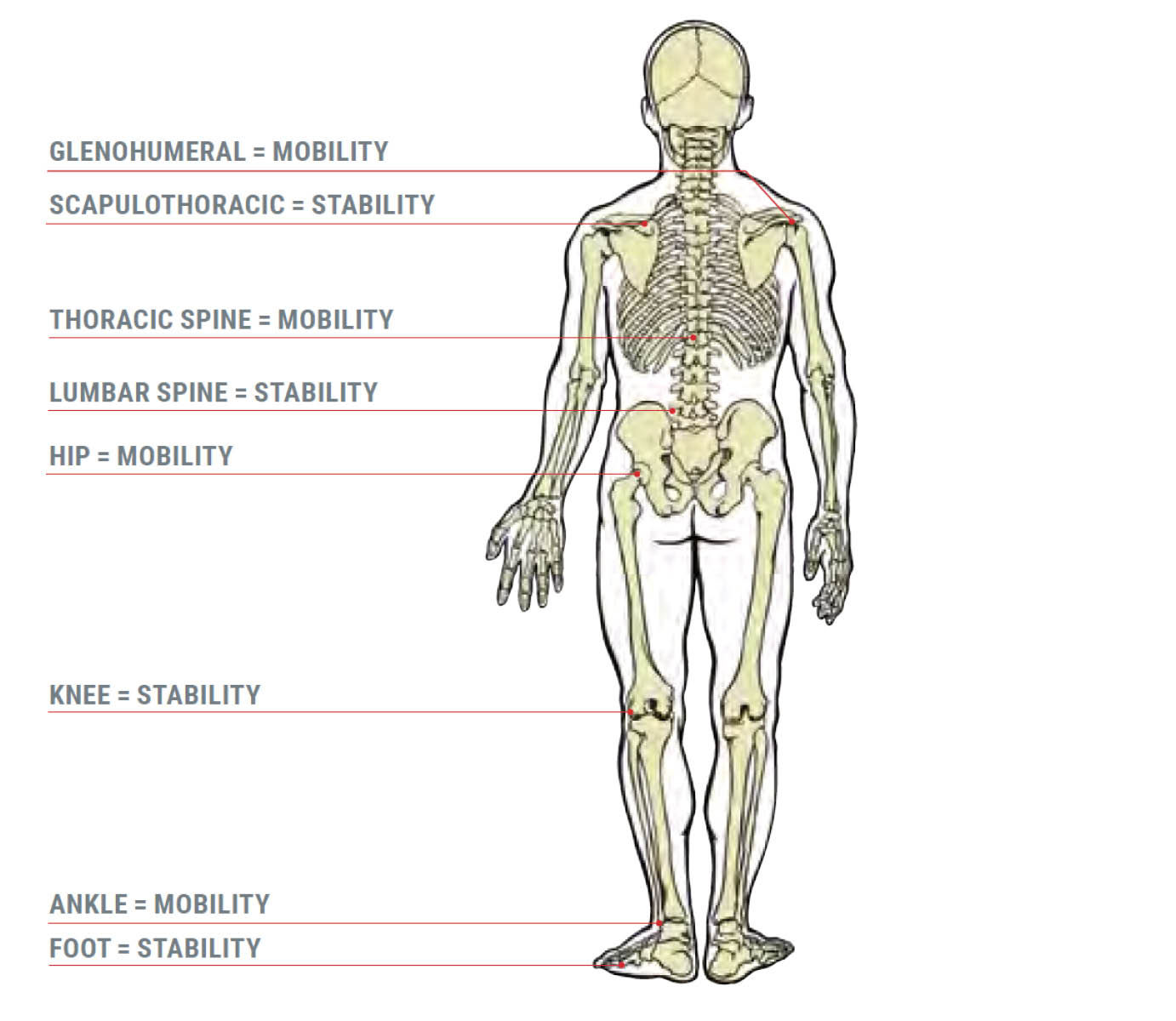
A useful way to think about mobility is through a joint-by-joint lens (Figure 1). Some regions are designed to be highly mobile, while adjacent regions are asked to provide more stability. Although every joint has both mobility and stability demands, the ankle and foot complex, hips, thoracic spine and glenohumeral joints generally need substantial movement capacity, while the knees, lumbar spine and scapulothoracic region often serve as important stabilizers during loaded tasks.
Figure 1. Mobility and Stability of the Kinetic Chain
Problems begin when the body loses motion at joints that are supposed to move. If the hips cannot extend or internally rotate effectively, the body may borrow motion from the lumbar spine during squatting, hinging or gait. If the thoracic spine cannot rotate or extend, the shoulder or low back may compensate during pressing, pulling or rotational work. If ankle dorsiflexion is limited, clients may collapse the foot, rotate the knee inward or reduce squat depth. Over time, these compensations can alter technique, distribute forces poorly and increase the likelihood of overuse syndrome.
This is why mobility training should be specific. Random stretching may feel good, but it does not necessarily restore the particular motion a client lacks or teach the body how to use that motion under load. Program design should focus on the regions most likely to limit movement quality:
Foot and ankle complex: Mobility here supports gait mechanics, squat depth and shock absorption. Limited dorsiflexion can change movement strategy all the way up the kinetic chain.
Hips: As a triplanar joint, the hip must flex, extend, abduct, adduct and rotate efficiently. Prolonged sitting often leaves clients short on hip extension and rotation.
Thoracic spine: Extension and rotation in the upper back help spare the lumbar spine and improve overhead mechanics.
Shoulder complex: Shoulder mobility depends on the coordinated motion of the glenohumeral joint, scapula and thoracic spine, not the shoulder joint alone.
Aging magnifies the importance of this work. With age, clients may experience reductions in muscle mass and strength, lower tolerance for high-force loading, more stiffness from repetitive postures or inactivity and, in some cases, degenerative joint changes. None of that makes mobility training optional; it makes it more relevant. When clients lose the strength to control ROM or avoid positions because they feel stiff, the available movement window narrows. Tasks that were once automatic—bending, rotating, stepping quickly or reaching overhead—begin to require more effort and more compensation. Mobility training helps counter that process by continually asking the nervous system and musculoskeletal system to maintain access to useful motion.
Importantly, mobility training does not mean forcing clients into end-range positions. The goal is to create comfortable, repeatable access to motion they can control. For some clients, that may mean starting with low-load floor-based patterns. For others, it may involve controlled multiplanar lunges, crawling patterns, transitions from the floor to standing or integrated warm-up drills. The correct dose is determined by function, not by how dramatic the stretch looks.
Programming Mobility and Flexibility for Client Success
For health and exercise professionals, the question is not whether to use flexibility training or mobility training. The question is when each tool is most appropriate. Passive flexibility work is useful when a client demonstrates clear tissue shortness, elevated resting tone, discomfort related to stiffness or a need to downshift after training. Static stretching can fit well during the cool-down, in a stand-alone recovery session or as part of a home-based program for areas that consistently limit ROM. It can also be valuable when an assessment suggests a client does not have enough passive range to access a position at all.
Mobility work should lead when the goal is movement preparation, movement re-education or improving technique in real exercise patterns. Before a workout, dynamic mobility drills can raise tissue temperature, increase circulation and prepare the nervous system for force production. More importantly, they can rehearse the movement qualities required for the session ahead. A lower-body day might emphasize ankle dorsiflexion, hip extension, hip rotation and trunk control. An upper-body day might emphasize thoracic extension and rotation, scapular upward rotation and controlled shoulder flexion.
Assessment should guide your decision making. If a client has passive range but cannot express it actively, prioritize strength and motor control within that range. If passive and active range are both limited, combine targeted flexibility work with mobility drills and loading strategies that gradually teach the client to own the new motion. This prevents a common programming mistake: adding more stretching to a control problem or adding more strengthening to a true range limitation without addressing the restriction.
One practical way to integrate mobility is to build it around the primary movement patterns clients need most: bending and lifting, single-leg patterns, pushing, pulling and rotation. These patterns reflect how people move in sport and daily life, and they allow you to train ROM in a way that is immediately useful. For example, a split-stance hip flexor mobility drill can progress into a lunge, while a quadruped thoracic rotation exercise can progress into a high-plank with thoracic rotation. Ankle rocks can progress into squat-to-stand patterns, while scapular control and thoracic mobility can progress into overhead reaching or pressing patterns. The progression matters because clients learn to access motion first, then control it, then apply it to increasingly functional tasks.
Mobility can also be programmed between sets as low-fatigue fillers. Between heavy hinges, for example, you might use a short hip-opening drill or a controlled transverse-plane lunge. Between pressing sets, thoracic rotation or wall slides may help restore position without creating excessive fatigue. This keeps clients engaged, adds high-quality repetition and can improve the next set rather than interfere with it.
Dedicated mobility sessions are also valuable, especially for deconditioned clients, older adults, clients returning from periods of inactivity and highly trained clients accumulating fatigue from repetitive training. A 20- to 30-minute session of low-to-moderate intensity body-weight mobility work can promote circulation, reduce stiffness and reinforce movement patterns without adding substantial recovery cost. Because these sessions are not intended to create high fatigue, they can often be used on the day after a strenuous workout as active recovery. Clients frequently report that they feel better once they start moving, which is consistent with the idea that gentle movement increases circulation, raises tissue temperature and reduces the sense of stiffness associated with inactivity or delayed-onset muscle soreness.
Daily exposure matters as well. Mobility is highly responsive to regular practice. Short “movement snacks” of five to 10 minutes can be enough to maintain joint motion and reinforce better movement options, particularly for clients who sit for long periods or perform the same tasks repeatedly. For many clients, consistency is more important than complexity. A small dose of controlled joint circles, hip mobility, thoracic rotation and loaded or unloaded patterning performed most days will usually outperform an occasional long session that is difficult to sustain.
Practical Programming Guidelines
A simple framework can help you decide how to use these tools in a client’s program:
Assess passive ROM and active control separately. A client may have one without the other.
Prioritize mobility at the joints that are meant to move, especially the ankles, hips, thoracic spine and shoulders.
Use controlled, pain-free ranges rather than forcing end-range positions.
Progress from simple to complex: floor to standing, unloaded to loaded, slow to faster and more reactive.
Match the method to the goal. Use static stretching to address tissue extensibility or downregulate after training; use mobility drills to prepare, teach and reinforce movement.
In the video below, ACE Certified Professional Pete McCall demonstrates a sample mobility program and shows you how to organize low-intensity body-weight exercises into an effective workout that enhances mobility, particularly in the hips and thoracic spine, two of the most mobile regions of the body. Loss of mobility in these segments could significantly impact the low back and knees and be a potential source of injury.
Conclusion
Flexibility and mobility should not be used as synonyms. Flexibility gives clients access to range; mobility lets them control it. For health and exercise professionals, that distinction sharpens assessment and programming. It explains why some clients need tissue-focused interventions, why others need motor-control and strength-based solutions, and why many need both. The more effectively you train mobility—especially at the ankles, hips, thoracic spine and shoulders—the more likely your clients are to move efficiently, tolerate training and maintain independence over time.
In practice, this means treating mobility as a foundational training quality, not as an afterthought. When clients learn to own their range of motion, movement becomes more efficient, exercise technique improves and daily tasks demand less effort. That is the real value of mobility work: not simply helping clients move more but helping them move well enough to keep doing the activities that matter most.
Sign up to receive CERTIFIED™
CERTIFIED™ is a free online monthly publication from ACE designed to equip certified fitness professionals and health professionals alike with the knowledge they need to continue growing.
Author
Pete McCall
Health and Fitness Expert
Pete McCall is the author of Ageless Intensity: High Intensity Workouts to Slow the Aging Process, Smarter Recovery: A Practical Guide to Maximizing Training Results, and Smarter Workouts: The Science of Exercise Made Simple. McCall is a personal trainer and fitness instructor at the exclusive Rancho La Puerta Resort and Spa in Tecate, Mexico, helping guests learn how to use strength training to achieve longevity. McCall holds a master’s degree in exercise science and health promotion, is a Certified Strength and Conditioning Specialist (CSCS) through the National Strength and Conditioning Association and has spent a large portion of his career educating personal trainers around the world as a workshop instructor and speaker. In addition to three books, Pete has authored numerous articles for fitness trade publications, exercise-science blogs and textbook chapters.
In an effort to help you more efficiently earn continuing education credits while you explore
CERTIFIED™, you can now take the quiz as you read. Get the latest, science-based information
while you earn 0.2 CECs.
Sign up to receive CERTIFIED™
CERTIFIED™ is a free online monthly publication from ACE designed to equip certified fitness professionals and health professionals alike with the knowledge they need to continue growing.




 by
by