
Lance C. Dalleck, PhD, Angela M. Dalleck, MSc, Bryant R. Byrd, MSc, Ryan M. Weatherwax, PhD, and Daniel J. Green
What You Need to Know
This is the first report on an ongoing three-year study examining the effectiveness of exercise programming based on the ACE Integrated Fitness Training® Model. The results of this study provide additional support to the findings of previous ACE-supported research on the Model—namely, that the personalized approach optimizes training responsiveness and positively impacts both cardiorespiratory fitness and cardiometabolic health.
Since first introducing the ACE Integrated Fitness Training® (ACE IFT®) Model more than a decade ago, ACE has been supporting research to investigate its effectiveness in real-world settings.
Previous research on the ACE IFT Model has shown the following:
- An individualized exercise program based on the ACE IFT Model elicited significantly greater improvements in VO2max, muscular fitness and key cardiometabolic risk factors. In addition, an individualized exercise program increased training responsiveness when compared to a standardized exercise training program.
- Exercise programming based on the ACE IFT Model is effective in a community setting in terms of reducing cardiovascular risk in adults, demonstrating that the results of the study mentioned above also can be seen when the Model is used on a larger scale. Also, these findings support the implementation of the Model as a means of community-wide primary prevention initiatives.
- Older individuals adapt to personalized cardiorespiratory and muscular training and improve health-related components of physical fitness to the same relative extent as younger individuals when adhering to a personalized exercise program based on the ACE IFT Model.
- The ACE Mover Method™—the cornerstone of the ACE IFT Model’s client-centered approach—is a successful strategy for facilitating behavior and lifestyle changes.
This current study represents the next step in this growing body of research. Like the studies cited above, this research was conducted by Lance Dalleck, PhD, and his team of researchers in the High Altitude Exercise Physiology Program at Western Colorado University. This is the first report on an ongoing randomized, controlled trial that will last three years. At the conclusion of this project, researchers will have conducted a multi-year, multi-site study that provides a robust body of data from more than 100 participants.
The purpose of the study is to examine the effectiveness of personalized exercise programming using the ACE IFT Model at eliciting favorable comprehensive training responsiveness (i.e., cardiorespiratory fitness + muscular fitness + cardiometabolic health). The findings presented here are from year 1 of this research.
The Study
Fifty-one nonsmoking men and women ranging in age from 42 to 80 years old were recruited to participate in a 13-week study. All were physically inactive, which is defined as not having participated in at least 30 minutes of moderate-intensity physical activity on at least three days of the week for at least three months, and all were asked to continue their current dietary habits and to not perform additional exercise beyond that required for the research. None of the participants had evidence of cardiovascular, pulmonary and/or metabolic disease, as determined by the completion of a medical history questionnaire.
The participants underwent two days of baseline measurements prior to the beginning of the study. The following variables were measured:
- Resting heart rate
- Resting blood pressure
- Anthropometric measurements: height, weight, percent body fat, and waist and hip circumferences
- Fasting blood lipids
- Fasting blood glucose
- Muscular fitness testing: five-repetition maximum (5-RM) for the bench press and leg press exercise
- Maximal exercise testing: maximal oxygen consumption (VO2max) and maximal heart rate [note that heart-rate reserve (HRR) was calculated for each participant by subtracting resting heart rate from maximal heart rate]
- First and second ventilatory thresholds (VT1 and VT2)
After completing the baseline assessments, the participants were randomized into three groups:
- ACE IFT Model group
- Standardized training group
- Control group
The Exercise Programs
The cardiorespiratory exercise was performed on various modalities: arm, cycle and rowing ergometers; elliptical crosstrainers; and treadmills. The standardized training group worked at an intensity based on a percentage of their HRR, while those in the ACE IFT Model group received programming based on their ventilatory thresholds. For both groups, a target heart rate was determined to coincide with either the HRR or ventilatory thresholds to establish a specific exercise intensity for each exercise session.
The cardiorespiratory training programs progressed for both groups over the course of the 13 weeks. Frequency remained consistent for both exercise groups, at three workouts per week throughout the study.
For the standardized training group, cardiorespiratory exercise began in week 1 at 40 to 45% of HRR for 25 minutes per day. The duration of each training session was extended by 5 minutes each week until weeks 5 and 6, when intensity increased to 50 to 55% HRR for 45 minutes per day. Then, in weeks 7 and 8, duration increased to 50 minutes per day. For the final five weeks of the study, this group exercised at 60 to 65% HRR for 50 minutes per day.
For the ACE IFT Model group, cardiorespiratory exercise began at a heart rate below VT1 for 25 minutes per day. As with the standardized training group, the duration of training sessions was extended by 5 minutes per week until weeks 5 and 6, when intensity increased to a heart rate greater than or equal to VT1 but below VT2. Then, in weeks 7 and 8, duration increased to 50 minutes per day. For the final five weeks of the study, this group exercised at an intensity greater than or equal to VT2 for 50 minutes per day.
Muscular Training
Muscular training was introduced during week 4 and continued to be performed three days per week through week 13.
For the standardized training group, the program consisted of the following single- and multijoint exercises performed on machines:
- Bench press
- Shoulder press
- Lat pull-down
- Seated row
- Biceps curl
- Triceps push-down
- Seated leg press
- Seated leg extension
- Prone leg curl
- Seated back extension/flexion
Two sets of 12 repetitions were completed for each exercise. Resistance was progressed every two weeks by approximately 3 to 5% of the total weight lifted for the upper body and approximately 6 to 10% for lower-body exercises. A session rating of perceived exertion (RPE) of 5 to 6 on the 0-to-10 scale was maintained across the training program.
For the ACE IFT Model group, muscular training consisted of multijoint/multiplanar exercises using both free weights and machines. The machines allowed for free motion during the exercises, meaning that range of motion was not limited to a specific arc. The following exercises were performed:
- Stability ball circuit (glute bridges, crunches, Russian twists, planks)
- Lunge matrix
- Kneeling/standing wood chops
- Kneeling/standing hay balers
- Dumbbell squat to 90-degree knee bend
- Standing one-arm cable row
- Step-ups with dumbbell onto a 6-inch (15-cm) step
- Modified (assisted) pull-ups
- Dumbbell bench press
Two sets of 12 repetitions were completed for each exercise. The intensity of weighted exercises started at 50% of 5-RM and was progressed by 5% 5-RM increments every two weeks. For exercises that did not include a weighted resistance (e.g., stability ball circuit), the number of repetitions was increased by approximately 5 to 10% to maintain an RPE rating of 5 to 6 on the 0-to-10 scale.
Figure 1 provides a flow chart of the experimental procedures and exercise programs for all three groups.
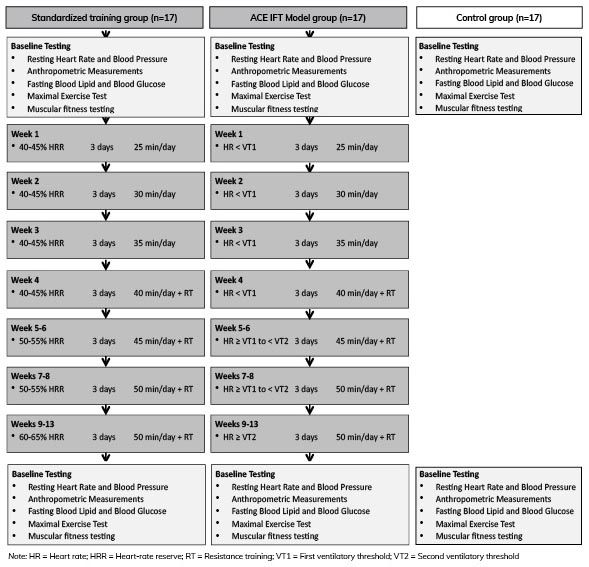
Figure 1. Flow chart of experimental procedures and exercise programming for each of the two exercise training groups
The Results
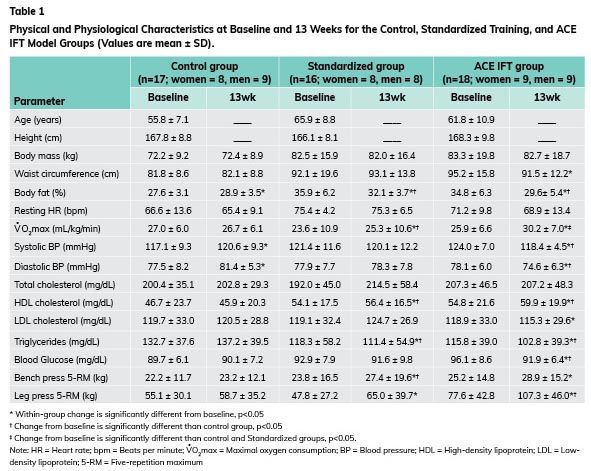
At the end of the 13-week program, participants from all three groups repeated the measurements taken at the outset. It is important to note that the three groups did not differ in physical or physiological characteristics prior to the study.
Here are the key findings, as presented in Table 1:
- Changes in VO2max were significantly more favorable in the ACE IFT Model group when compared to the standardized training group and control group.
- Changes in body mass, waist circumference, resting heart rate and total cholesterol were not significantly different in either the standardized training or ACE IFT Model groups.
- Changes in body-fat percentage, systolic and diastolic blood pressure, high-density lipoprotein (HDL) cholesterol, triglycerides, blood glucose and leg press 5-RM were significantly more desirable in the ACE IFT Model group relative to the control group.
- Changes in VO2max, body-fat percentage, HDL cholesterol, triglycerides and bench press 5-RM were significantly more desirable in the standardized training group when compared with the control group.
Another element of the findings of this research centers on the incidence of VO2max non-responders and responders, which you can learn more about in this ACE-supported 2017 study on the ACE IFT Model. As you can see in Figure 2A, 62.5% of those in the standardized training group experienced a favorable change in VO2max, which categorized them as responders. This leaves 37.5%, or six of the 16 individuals in this group, experiencing an undesirable change in VO2max. Meanwhile, in the ACE IFT Model group (Figure 2B), 100% of participants saw a positive improvement in VO2max. Importantly, there were no significant differences between these two groups in several potential influencing factors on responders/non-responders, including age, baseline VO2max, exercise adherence and sex.
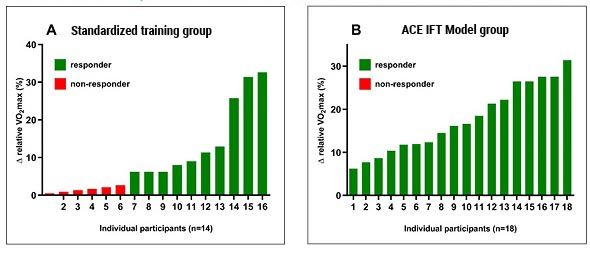
Figure 2. Individual variability in relative VO2max response (% change) to exercise training in the standardized training (A) and ACE IFT Model (B) groups
The Bottom Line
The results of this study provide additional support to the findings of previous ACE-supported research on the ACE IFT Model—namely, that the personalized approach made possible by the Model optimizes training responsiveness. As explained by Dr. Dalleck, “Participants in the group that followed the ACE IFT Model programming all had significant improvements in both cardiorespiratory fitness and cardiometabolic health.”
In addition, Dr. Dalleck says, “This study confirmed what previous research found, that by personalizing programming through the ACE IFT Model, you’re getting a lot more uniformity in terms of the response to training. You’re not having the incidence of non-responders that you have with standardized, generic training.”
As this ongoing study continues over the course of the next two years, examining the effectiveness of personalized exercise programming using the ACE IFT Model at eliciting favorable comprehensive training responsiveness (i.e., cardiorespiratory fitness + muscle fitness + cardiometabolic health), ACE will continue to report on its findings.
So, what does this research mean to you, the ACE Certified Professional?
Given that the primary mission of the American Council on Exercise is to get people moving, it is paramount that health and exercise professionals have evidence-based programming options available to implement at the individual and community levels. These preliminary findings are encouraging. At the conclusion of this three-year project, it is anticipated that this study and its findings will provide robust evidence for the efficacy of personalized exercise programming using the ACE IFT Model. Furthermore, it is our vision that these findings could also underpin future iterations of exercise guidelines at the national and international level.
Exercise Programming: Muscular Training and the ACE IFT Model
With an understanding of its Muscular Training component, you can use the ACE IFT Model as a guide to develop safe and effective periodization plans that help your clients reach their muscular-training goals.
In this video training, you will closely examine the Muscular Training component of the ACE IFT Model and learn how to move through its phases. You will also learn how to plan out long-term exercise programs and gain your client’s trust by keeping them safe and educating them on the process.
Led by Michelle Leachman, CORE Health and Fitness and ACE Master Trainer who has been teaching and publishing research on human anatomy, physiology and exercise science, you will walk away with the skills to apply the ACE IFT Model Exercise Programming Template to any client’s individual muscular-training goals.
Upon completion, you will be able to:
• Leverage the phases of the Muscular Training component of the ACE IFT Model
• Safely move a client from one phase to the next, progressing from Functional to Movement to Load/Speed Training
• Understand long-term application of the Muscular Training component phases and apply them to clients who have goals in this area
• Apply three separate training plans using the ACE IFT Model’s Muscular Training component
This study, which was commissioned by the American Council on Exercise, was first published in the peer-reviewed
International Journal of Research in Exercise Physiology.




 by
by 



