Can Reduced-exertion High-intensity Interval Training Combat the Harmful Effects of a Sedentary Lifestyle?

Certified™: Research Special Issue

Lance C. Dalleck, PhD, Morgan J. Berryman-Maciel, MSc, Lai Ling Yeung, BSc, and Logan Negley, BSc, with Daniel J. Green
“I just don’t have time to exercise on a regular basis.”
How many times have you heard this from clients or potential clients? And how many times have you stated it yourself?
Considering that lack of time is often cited as a barrier to exercise, it’s no wonder exercise physiologists and equipment manufacturers are on an ongoing quest to develop ways to achieve the benefits of exercise in shorter periods of time.
The impact to be made by maximizing the benefits of short-duration workouts cannot be overstated. Physical inactivity plays a prominent role in the development of type 2 diabetes and other health-related diseases, including metabolic syndrome (MetS) and cardiovascular disease (Ruffino et al., 2016). More than 422 million people worldwide have type 2 diabetes (Ruffino et al., 2016), including 30.3 million people in the United States (Centers for Disease Control and Prevention, 2017), and increasing the physical-activity levels of these individuals can help prevent or delay the course of disease (Howden et al., 2018)—not to mention the preventive benefits of physical activity for people with prediabetes.
Some researchers and manufacturers, including the developers of the CAR.O.L stationary bike (see sidebar), believe reduced-exertion high-intensity interval training (REHIT) may be the key to overcoming the “lack of time” barrier to regular exercise.
REHIT is an evolution of high-intensity interval training (HIIT), which is seen as a time-saving alternative to traditional moderate-intensity cardiorespiratory exercise. While HIIT has been shown to have many of the same benefits of traditional cardiorespiratory exercise, the sessions still last 30 minutes and are associated with high rates of perceived exertion, making them a less suitable option for individuals who are currently sedentary or battling disease.
REHIT programming shortens that duration and creates a workout that doesn’t feel quite so tough, both of which may positively impact long-term adherence. This approach consists of two or three 10- to 20-second sprints within a 10-minute session. According to Metcalfe et al. (2015), significant glycogen depletion occurs within 10 to 20 seconds of a supramaximal sprint, which has been shown to have a positive effect on several health parameters, including insulin sensitivity. This shorter, less-intense alternative to HIIT programming provides sedentary populations a way to easily incorporate exercise into their daily routines, reap health benefits and develop positive exercise habits.
The CAR.O.L Bike
CAR.O.L (CARdiovascular Optimization Logic), formerly known as High Octane Ride, is a stationary bike that incorporates REHIT programming. According to the manufacturer’s website, the bike uses a form of artificial intelligence that controls the resistance and timing on the rides and adjusts the resistance to each individual’s level of both power and fatigue, helping him or her get progressively fitter and stronger.
ACE enlisted the help of Lance Dalleck, PhD, and his team of researchers in the High Altitude Exercise Physiology Program at Western Colorado University to determine if three weeks of REHIT workouts on the CAR.O.L bike was enough to overcome the negative cardiometabolic effects of a sedentary lifestyle.
The Study
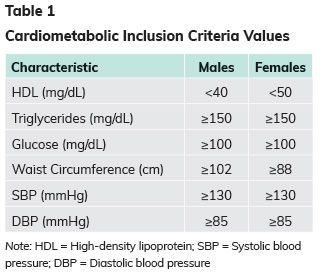
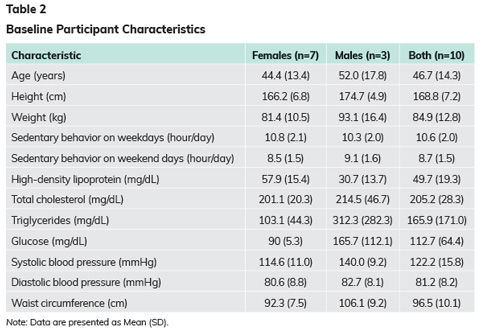
The research team recruited 10 volunteers for this study, all of whom were sedentary for eight or more hours per day, had two cardiometabolic risk factors for MetS (Table 1), and were able to exercise on a treadmill and stationary bike. None of the participants were pregnant and all were between the ages of 18 and 64 years. The participants’ baseline characteristics are presented in Table 2.
Prior to the beginning of the study, all participants underwent comprehensive baseline testing, including the following parameters: International Physical Activity Questionnaire (IPAQ) to determine physical-activity levels, maximal oxygen uptake (VO2max), resting blood pressure and heart rate, waist circumference, body weight, dual-energy x-ray absorptiometry (DXA) to determine body composition, fasting insulin, fasted glycosylated hemoglobin (HbA1c), fasting blood lipids and fasting glucose.
Participants were then randomly assigned to either the REHIT group or a control group for the first three weeks of the six-week study. After three weeks, the participants switched groups.
The REHIT group rode the CAR.O.L bike three times each week for 9 minutes and 40 seconds, including a warm-up, cool-down and two all-out sprints separated by a 3-minute recovery period. The bike’s software coaches the participant through each workout with written and verbal cues of when and how long to sprint and offers tips on proper breathing and recovery techniques.
Both groups were asked to maintain their normal diets and the REHIT group was asked to maintain their activity levels outside of the workout sessions.
The testing described above was repeated after weeks 3 and 6 (i.e., after each group completed its role as the REHIT group and the control group). After weeks 1, 2, 4 and 5, all participants underwent testing consisting of measurements of physical-activity levels (IPAQ), resting blood pressure and heart rate, waist circumference, weight, fasting blood lipids and fasting blood glucose.
The Results
Four of the participants did not complete all nine rides during the three-week period for various reasons not related to the study itself. While all 10 participants completed the comprehensive testing before week 1 and after weeks 3 and 6, one participant missed a weekly testing session during the control period and two participants missed a weekly testing session during the REHIT period. Any participant who completed fewer than seven rides was excluded from the results calculations.
The physiological characteristics of both groups before and after the study are presented in Table 3.
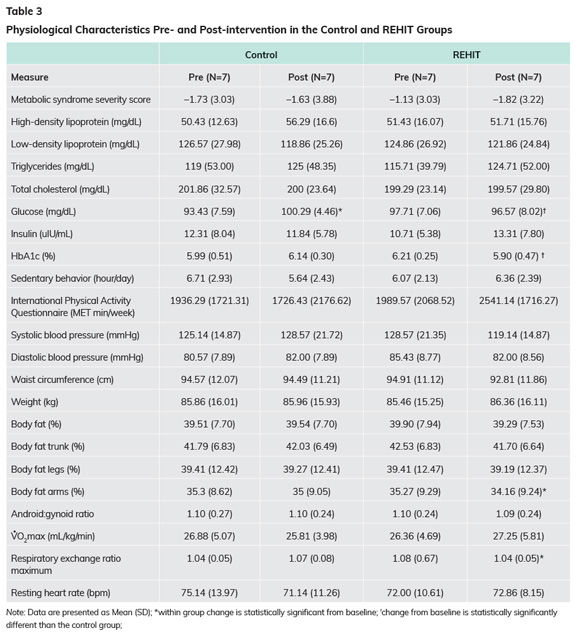
So, what does all of this data mean?
This study found that after three weeks of three REHIT sessions per week, fasting blood glucose and HbA1c decreased significantly when compared to the control group in a sedentary, MetS-affected population.
While MetS z-scores*, systolic blood pressure and waist circumference were notably decreased in the REHIT group, these changes were not statistically significant. According to the research team, the mean reduction in MetS z-score by 0.69 after three weeks of time-efficient, workplace-based training (the bike was placed near the participants’ workplace, allowing them to break up their sedentary behavior during the workday) provides promising evidence for the usefulness of REHIT as an exercise recommendation for MetS-affected populations.
* Note: The MetS z-score is a means of measuring training responsiveness that combines a number of cardiometabolic risk factor values into a single continuous score. These values include blood pressure, circumference measures, blood glucose, high-density lipoprotein and triglycerides (Malin et al., 2013). The primary benefits for inclusion of a continuous MetS z-score are twofold: (1) it acknowledges that there is a continuum to cardiometabolic risk within each individual and (2) it provides a more sensitive tool for assessing individualized training responsiveness following an exercise intervention.
There were no statistically significant changes in cardiorespiratory fitness, which is hardly surprising for such a short intervention. Notably, the researchers observed a positive trend toward improved VO2max values in the REHIT group. Also, these previously sedentary participants may not have been able to exercise at very high intensities, meaning that they may not have been working hard enough to elicit improvements in VO2max due to a lack of physical fitness.
While changes in anthropometric measures were not statistically significant, average body-fat percentage and waist circumference did decrease in the REHIT group.
The Bottom Line
Dr. Dalleck points out that the cardiometabolic values all improved over the course of this short study but offers an important caveat: “These are very exciting findings for such a short time commitment, but that doesn’t mean that people should replace their regular exercise programs with a REHIT program. Instead, REHIT can be used as a strategy during busy periods to avoid the detraining effects of lapses in exercise.”
In other words, REHIT programming is a great approach for personal trainers to use with clients that is time-efficient, self-guided and personalized—which may be the perfect solution when life gets busy. Remember, having a plan for foreseeable lapses in clients’ routines may be part of the solution for maintaining long-term exercise adherence.
Finally, this study found that a workplace-based, time-efficient REHIT program was well-tolerated by sedentary individuals possessing MetS risk factors. Companies that want to invest in their employees’ wellness could purchase a bike similar to the one utilized in this study to provide employees with a time-efficient way to interrupt their sedentary behavior during the workday. REHIT could also provide sedentary populations a way to “get moving” and develop an enjoyment for exercise, which could potentially lead to better exercise adherence in the long run.
References
Centers for Disease Control and Prevention (2017). Cholesterol.
Howden, E.J. et al. (2018). Reversing the cardiac effects of sedentary aging in middle age—a randomized controlled trial. Circulation, 137, 15, 1549−1560.
Malin, S.K. et al. (2013). Metformin modifies the exercise training effects on risk factors for cardiovascular disease in impaired glucose tolerant adults. Obesity, 21, 93−100.
Metcalfe, R.S. et al. (2015). Physiological and molecular responses to an acute bout of reduced-exertion high-intensity interval training (REHIT). European Journal of Applied Physiology, 115, 11, 2321–2334.
Ruffino, J.S. et al. (2016). A comparison of the health benefits of reduced-exertion high-intensity interval training (REHIT) and moderate-intensity walking in type 2 diabetes patients. Applied Physiology, Nutrition, and Metabolism, 42, 2, 202–208.