Carbohydrates fuel high-intensity training and performance, and yet questions have emerged regarding the role of carbohydrate in the diet of an athlete, particularly for those who desire both performance and a lean physique. Specifically, some have proposed that limiting carbohydrate might allow the body to better use other macronutrients as fuel, while still supporting enhanced performance yet creating a leaner physique.
This article examines the scientific evidence for using carbohydrate to support high-intensity exercise, the specific form of training that yields both performance enhancement and a more sculpted physique. The concept of planning an individual’s fueling for training separate from daily food intake allows for a strategic use of carbohydrate based on fueling needs, and an acknowledgement of the benefits of alternative fueling for lower-intensity and non-training days*.
Note: It is outside the scope of practice of a fitness professional to make speciffic recommendations or programming for nutrient or nutritional intake, caloric intake or specialty diets. The information provided in this article should be used to help inform clients about current research, not to make specific nutritional recommendations. Check out A Call to Lead: Why Fitness Professionals Should Discuss Nutrition With Their Clients for more information on ACE's Position Stand on Nutrition Scope of Practice for Fitness Professionals.
Historical Perspective
Medical practitioners have been experimenting with the influence of dietary factors on health and disease for centuries. Beginning in 500 BC and then again in the 1920s, the ketogenic diet (a high-fat, low-carb dietary approach that forces the body to burn fat instead of carbohydrate and brings about a state of elevated ketones known as ketosis) and related dietary treatments were tested for their effect on controlling epileptic seizures, with some success seen in responsive subjects and patients (Rho 2015).
In the 1930s, the safety and efficacy of very-low-calorie diets (VLCD) were investigated as a viable treatment for obesity. Dietary treatments of 25 to 30 grams of carbohydrate and 200 to 400 kilocalories per day led to a weight loss of approximately 4½ pounds (2 kg) per week, but these treatments were very difficult for subjects to maintain after the inpatient portion of the studies (Howard, 1981).
The mid-1960s changed the way we thought about fueling muscle cells. Jonas Bergstrom and Eric Hultman discovered glycogen supercompensation, which is the ability of the muscle cell to store a greater amount of glycogen. The research went on to show that glycogen supercompensation enhanced the performance of heavy exercise (Bergstrom et al., 1967; Bergstrom and Hultman 1966).
The link between chronic disease and physical inactivity also emerged in the 1960s. That link led researchers to study the impact of carbohydrate-containing and carbohydrate-restricted hypo-caloric diets on weight loss in obese sedentary subjects placed on an exercise regimen. After six weeks, the outcome showed no difference in weight loss or body-composition changes between groups. Importantly, endurance decreased by 50 percent in the subjects on the carbohydrate-restricted diet, and muscle glycogen data correlated well with percent changes in endurance (Bogardus et al, 1981).
A leap in our understanding of fueling for moderate-intensity exercise occurred in 1983, with the publication of a study showing the preservation of submaximal exercise capability with reduced carbohydrate oxidation in elite cyclists following a ketogenic diet (KD) for 28 days (Phinney et al., 1983). Although subjects could maintain exercise levels of 65 percent of VO2max on the KD diet, sprint capability remained constrained during the period of carbohydrate restriction. According to lead researcher Dr. Phinney, “…anaerobic (i.e., weight lifting or sprint) performance is limited by the low muscle glycogen levels induced by a ketogenic diet, and this would strongly discourage its use under most conditions of competitive athletics” (Phinney, 2004).
More recently, studies have returned to investigating the influence of carbohydrate on fat loss and weight-loss maintenance in overweight and obese subjects. While some data support faster weight loss in carbohydrate-restricted diets, this result and the ability to maintain the weight loss only applies to those who can sustain the diet over time. Furthermore, the healthiness of this diet style long-term is still controversial (Ebbeling et al., 2012) Additional studies investigating the influence of the KD as treatment for chronic diseases may show merit (Paoli et al, 2013).
Fueling Athletic Training
You don’t have to be a competitive athlete to train athletically. An athletic challenge pushes the body physically into levels of high-intensity exercise. We learned in the 1960s that this training requires carbohydrate fuel, and it has been confirmed by our current knowledge of muscle physiology (van Loon et al., 2001). It is during the high-intensity levels of training, at greater than 70 percent VO2max, where the greatest training effect occurs. This is also when the greatest proportion of calories are burned per minute during exercise, and results in the greatest energy requirements for excess post-exercise oxygen consumption (EPOC), when fat-oxidation is highly elevated. High-intensity interval and strength training place a greater demand on the anaerobic energy pathways during the workout, increasing the need for oxygen after the workout and enhancing EPOC (LaForgia et al., 2006; Bersheim and Bahr 2003). This is when the body’s muscles are sculpted in addition to being trained.

Many athletes and clients desire an aesthetic benefit from their training. The dual goals of performance and sculpting have led to the dietary fads of under-fueling and carbohydrate restriction in what are assumed to still be performance-enhancing diets. But both assumptions are false. Every study has shown diminished athletic performance from a carbohydrate-restricted or KD compared to a carbohydrate-rich diet in athletes (Kleiner, 2015). Moreover, very-low-carbohydrate dieting has a profound influence on health, especially in highly active individuals and in women. Immune function (Gleeson and Bishop, 2000), insulin sensitivity, inflammation (Asrih et al., 2015), gut biome changes (Duncan et al., 2007), carbohydrate and brain activity (Rattray et al., 2015), and the peripheral metabolic pathway (Cooper, 2014) are all compromised when high demands are made on energy systems without adequate carbohydrate substrate availability. Under these circumstances physiological processes are suppressed by severely low energy availability, and measurement of total or resting energy expenditure will underestimate energy requirements (Loucks et al., 2011).
New concepts separating the daily physiological energy demands from fueling demands for training can improve estimates for energy availability. Because energy output decreases when energy needs are not met, an estimate of energy balance does not give a true reflection of energy needs. The energy deficit creates a false artifact of a stunted energy demand. To maximize training, a registered dietitian or qualified professional can determine the true energy needs of training in the fully fueled athlete or client. If a client is seeking both performance and sculpting results, he or she can create a small deficit during meals of 300 to 400 total calories per day to sustain metabolic rate. The client should fully fuel training before and during a workout, and fully fuel recovery afterward.
Fueling Strategies
Never under-fuel training. Only fully fueled training results in an optimal workout and maximal results for both training effect and sculpting. Athletic people are notoriously under-fueled. It is really hard to fully fuel yourself and still be empty enough to train.
When training sessions involve high-intensity activity, carbohydrate will maximize the workout time, so that the athlete is fully fueled all the way to the end of exercise. Seventy-five to 90 percent of total fuel substrate calories will be carbohydrate during this type of workout. This will raise EPOC and result in better body sculpting, while also enhancing physical performance. Training sessions that focus on low-to-moderate intensity endurance for cardiorespiratory training require less carbohydrate fuel. In other words, if your client is hardly training on a particular day, he or she can consume less carbohydrate. Rest days are easy—don’t add training fuel.
Work closely with clients to find the right sports fuel for them. Proper fueling volume does not always allow for gastrointestinal comfort. Some products may be better tolerated than others. Some clients find that conditioning their gut to the use of sports fuel takes time. Experiment with different brands, ingredients, flavors, unflavored, volumes and timing. There are big differences between products, and few products have research data supporting the claims their manufacturers make. As a certified fitness professional, you should practice from an evidence-based position in all your guidance and recommendations, while also making sure to stay well within your scope of practice.
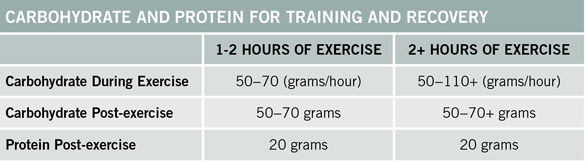
Carbohydrate and Protein Recommendations for Training and Recovery
With the help of a registered dietitian or a qualified nutrition professional, your performance-oriented clients should determine their caloric needs of training and recovery, and prioritize the use of carbohydrate and protein around exercise. To facilitate performance enhancement and sculpting, they should consider creating a 300- to 400-calorie deficit from starch-rich food, and schedule carbohydrate calories for fueling training.
References
Asrih, M. et al. (2015). Ketogenic diet impairs FGF signaling and promotes differential inflammatory responses in the liver and white adipose tissue. PLoS One, 10, 5, e0126364.
Bergstrom, J. and Hultman, E. (1966). Muscle glycogen synthesis after exercise: An enhancing factor localized to the muscle cells in man. Nature, 210, 5033, 309-310.
Bergstrom, J. et al. (1967). Diet, muscle glycogen and physical performance. Acta Physiologica Scandinavia, 71, 2, 140-150.
Bersheim, E. and Bahr, R. (2003). Effect of exercise intensity, duration and mode on post-exercise oxygen consumption. Sports Medicine, 33, 14, 1037-1060.
Bogardus, C. et al. (1981). A comparison of carbohydrate-containing and carbohydrate-restricted hypocaloric diets in the treatment of obesity. Endurance and metabolic fuel homeostasis during strenuous exercise. The Journal of Clinical Investigation, 2, 399-404.
Cooper, E. (2014). The Metabolic Storm. Seattle, Wash.: Seattle Performance Medicine.
Duncan, S.H. et al. (2007). Reduced dietary intake of carbohydrates by obese subjects results in decreased concentrations of butyrate and butyrate-producing bacteria in feces. Applied and Environmental Microbiology, 73, 4, 1073-1078.
Ebbeling, C.B. et al. (2012). Effects of dietary composition on energy expenditure during weight-loss maintenance. Journal of the American Medical Association, 307, 24, 2627-2634.
Gleeson, M. and Bishop, N.C. (2000). Elite athlete immunology: Importance of nutrition. International Journal of Sports Medicine, Supplement 1, S44-50.
Howard, A.N. (1981). The historical development, efficacy and safety of very-low-calorie diets. International Journal of Obesity, 5, 3, 195-208.
Kleiner, S.M. (May 1-2, 2015). Optimizing Nutrition for Performance. Keto- vs. Carb-Adapted: The whole story, including the holes. Presentation at The Fitness Summit, Kansas City, Mo.
LaForgia, J. et al. (2006). Effects of exercise intensity and duration on the excess post-exercise oxygen consumption. Journal of Sports Sciences, 24, 12, 1247-1264.
Loucks, A.B. et al. (2011). Energy availability in athletes. Journal of Sports Sciences, 29 Supplement, 1, S7-S15.
Paoli, A. et al. (2013). Beyond weight loss: A review of the therapeutic uses of very low carbohydrate (ketogenic) diets. European Journal of Clinical Nutrition, 67, 789-796.
Phinney, S.D. (2004). Ketogenic diets and physical performance. Nutrition and Metabolism, 1, 2.
Phinney, S.D. et al. (1983). The human metabolic response to chronic ketosis without caloric restriction: physical and biochemical adaptation. Metabolism, 32, 8, 757-768.
Rattray, B. et al. (2015). Is it time to turn our attention toward central mechanisms for post-exertional recovery strategies and performance? Frontiers in Physiology, 6, 79.
Rho, J.M. (2015). How does the ketogenic diet induce anti-seizure effects? Neurotic Letter, doi: 10.1016/j.neulet.2015.07.034 [Epub ahead of print].
van Loon, L.J.C. et al. (2001). The effects of increasing exercise intensity on muscle fuel utilization in humans. Journal of Physiology, 536, 1, 295-304.
______________________________________________________________________________




 by
by