High-intensity interval training (HIIT) involves alternating brief bouts of higher-intensity sessions with either rest or lower-intensity workloads throughout an exercise routine. While HIIT has traditionally encompassed aerobic modalities, recent research has begun to explore the application of HIIT to resistance exercise. The following article examines this unique form of strength training and how health and fitness professionals can safely and effectively integrate it into their clients’ programs.
What is Resistance-exercise HIIT?
As a health and fitness professional, you know that the number one excuse people give for not exercising regularly is lack of time. Arguably, this is a primary reason why HIIT has grown so popular over the past several years—great results in less time. Likewise, HIIT has captivated the attention of many researchers due to its superior ability to improve cardiorespiratory fitness (Weston, Wisløff and Coombes, 2014) and vascular function (Ramos et al., 2015) for a lesser weekly time-commitment relative to the current exercise guideline of moderate-intensity continuous training (MICT).
HIIT, which is characterized by short bursts of high-intensity training separated by periods of active or passive recovery (Kessler, Sisson, and Short, 2012), makes it possible for unfit individuals to accumulate periods of intense exercise that would otherwise not be possible if executed continuously. While HIIT is generally associated with aerobic activity, resistance exercise can also be effectively performed as HIIT by alternating brief bouts of higher-intensity sessions with either rest or lower-intensity workloads throughout the exercise training session.
A growing body of research on the application of HIIT to resistance exercise has yielded impressive preliminary findings. Here are five key studies:
1. A group of Italian and Greek researchers (Paoli et al., 2012) investigated the acute effects of resistance-exercise HIIT vs. traditional resistance exercise training on metabolism in a group of healthy, resistance-trained men (mean age = 28 years). The HIIT resistance exercises included the bench press, lat pull-down and leg press. The resistance-exercise HIIT group completed three series of six-repetition maximum (6-RM) followed by rest for 20 seconds. The participants subsequently lifted the same weight until reaching the point of failure (approximately two repetitions) followed by 20 seconds of rest and then another two to three repetitions. This entire sequence counted as one set. The participants then rested for two-and-a-half minutes before performing two additional sets. The leg exercise included three sets with two-and-a-half minutes of rest between sets. The two upper-body exercises consisted of two sets. The resistance-exercise HIIT session lasted approximately 32 minutes (including the warm-up period).
The traditional resistance exercise-training group performed four sets of eight different weightlifting exercises, including the bench press, lat pull-down, military press, biceps curls, triceps extensions, leg press, leg curls and sit-ups. The intensity of each lift was set between 70 and 75 percent of 1-RM. Participants were instructed to perform as many repetitions as possible in a set (approximately eight to 12 repetitions). They then rested for one minute between sets for single-joint exercises and two minutes for multiple-joint exercises. The traditional resistance exercise-training session lasted approximately 62 minutes (including the warm-up period).
Researchers found that following traditional resistance exercise training, participants’ resting energy expenditure and fat oxidation were unchanged 24 hours later. In comparison, following resistance-exercise HIIT, resting energy expenditure increased 23.7 percent and fat oxidation increased 3.5 percent. Researchers also concluded that the shorter exercise time commitment of resistance-exercise HIIT may help to reduce the “lack of time” barrier to regular exercise training.
2. A collaboration between New Zealand, Australian and British researchers (Francois et al., 2014) compared the effectiveness of acute bouts of combined resistance exercise/aerobic HIIT to aerobic HIIT alone in young- to middle-aged adults (age range = 18 to 55 years) who were insulin resistant. The resistance exercise/aerobic HIIT program consisted of six interval bouts of 60 seconds interspersed with 60 seconds of active recovery. The modality of HIIT alternated between resistance exercise and aerobic exercise, with three interval bouts of each. Participants performed resistance-exercise HIIT with resistance bands and targeted the musculature of the arms, back and core. The intensity of resistance-exercise HIIT bouts involved participants completing as many repetitions as possible within 60 seconds. The aerobic HIIT consisted of inclined treadmill walking at 90 percent of maximal heart rate. The aerobic HIIT alone group completed six interval bouts of 60 seconds of inclined treadmill walking at 90 percent of maximal heart rate interspersed with 60 seconds of active recovery. Researchers found that glucose control improved similarly in both the resistance exercise/aerobic HIIT group (10.3 percent) and the aerobic HIIT alone group (7.8 percent).

3. Canadian researchers (Francois et al., 2016) compared the effectiveness of an acute bout of resistance-exercise HIIT to aerobic HIIT in older adults (age range = 40 to 66 years) with and without type 2 diabetes. The resistance-exercise HIIT program featured seven resistance exercise interval bouts of 60 seconds interspersed with 60 seconds of active recovery. The resistance-exercise HIIT bouts were performed at a weight that elicited a rating of perceived of exertion (RPE) equal to 5 (or “hard”). Participants completed as many repetitions as possible in the 60-second bout. Active recovery involved walking to the next resistance-exercise station, which included the leg press, leg extension and hamstrings curl. Researchers concluded that following resistance-exercise HIIT, endothelial function improved 4 percent among participants with type 2 diabetes and 2 percent among non-type 2 diabetic older adults. Given that endothelial dysfunction is an early indicator of many chronic diseases, these findings have important long-term preventive implications.
4. A group of American researchers (Wingfield et al., 2015) investigated the acute effects of resistance-exercise HIIT on post-exercise oxygen consumption (EPOC) in a cohort of recreationally active women (mean age = 25 years). The resistance-exercise HIIT program featured six resistance exercises: the leg press, bench press, lunges, shoulder press, biceps curl and triceps extension, and consisted of three sets of 6-RM to 8-RM followed by 20 to 30 seconds of rest for each exercise. Participants rested for two-and-a-half minutes between each exercise, and the entire session lasted approximately 25 minutes. The researchers reported that EPOC increased 7.6 percent at 30 minutes and 2.5 percent at 60 minutes. Given the potential contribution of EPOC to weight loss and weight maintenance, these findings have important practical application for health and fitness professionals.
5. A group of American and British researchers (Giessing et al., 2016) investigated the chronic effects of resistance-exercise HIIT vs. traditional resistance exercise training on various markers of muscular performance and body composition in a group of healthy, recreationally active men and women (mean age = 22 years). The resistance-exercise HIIT group completed one set of each of the following exercises: chest press, heel raise, rear deltoid, elbow flexion, seated row, knee extension, knee flexion, abdominal flexion and push-ups. Each set consisted of repetitions to the point of momentary muscular failure (MMF) followed by two drop-sets in which the weight was reduced by 10 to 15 percent and repetitions were again performed to MMF (usually about two to three repetitions). Rest between each exercise consisted of enough time for participants to walk to the next exercise and resume normal breathing. Training load was progressed by 5 percent once participants could attain 15 repetitions to MMF. Participants completed the resistance-exercise HIIT two times per week for 10 weeks.
The traditional resistance exercise-training group performed the same exercises as the resistance-exercise HIIT group and completed three sets of each exercise with a rest period of two to three minutes between sets. Repetitions were performed to a self-determined RM (the specific intensity was not reported). Participants completed the traditional resistance exercise-training program two times per week for 10 weeks.
While neither group improved in any of the body-composition indices that were assessed, both groups increased their muscular performance score for each of the nine different exercises performed with the exception of push-ups. Moreover, the resistance-exercise HIIT group had greater muscular performance gains for heel raise, elbow flexion and knee flexion when compared to the traditional resistance-training group. The researchers concluded that muscular performance gains may be greater with resistance-exercise HIIT.
Collectively, these findings suggest that resistance-exercise HIIT may serve as an effective time-efficient substitute to commonly recommended traditional resistance-exercise training.
How to Integrate Resistance-exercise HIIT Into Your Clients’ Exercise Programs
The first issue that must be addressed prior to integrating a resistance-exercise HIIT program into the overall exercise program is safety. Overall, properly performed exercise is harmless for most people. In fact, there is greater risk associated with remaining physically inactive when compared to commencing with regular exercise training. The absolute risk of sudden death during vigorous-intensity physical activity has been estimated to be one per year for every 15,000 to 18,000 people (ACSM, 2014). In terms of the specific risk associated with HIIT, one study concluded that after 129,456 hours of moderate-intensity exercise and 46,364 hours of high-intensity exercise in 4,846 high-risk participants, there was one fatal and two non-fatal cardiac arrests. The authors concluded that the risk of a cardiovascular event with HIIT was low (Rognmo et al., 2012).
Pre-participation Screening
The key to minimizing complications during and after exercise is to identify those individuals who may be at an increased risk for adverse symptoms through appropriate pre-participation screening. The risk of an acute myocardial infarction or sudden death during exercise is higher in older adults relative to their younger counterparts. The greatest risk exists for those individuals with underlying or diagnosed cardiovascular disease. It must be assumed that any individual with a clinically relevant cardiovascular disease risk factor or diagnosed cardiovascular disease requires both a medical examination and physician-supervised maximal exercise test prior to participation in resistance-exercise HIIT (ACSM, 2014). These procedures will pinpoint contraindications to resistance-exercise HIIT. For example, an individual who terminates a maximal exercise test prematurely due to chest discomfort or dizziness would not be a candidate for resistance-exercise HIIT.
Ideally, health and fitness professionals should provide clients with a detailed description of the resistance-exercise HIIT program that can be reviewed and approved by client’s physicians. An appreciation for the potential risk involved with resistance-exercise HIIT coupled with a clear understanding of the importance for comprehensive screening prior to client participation in resistance HIIT are vital measures in risk management.
Resistance-exercise HIIT Program Design
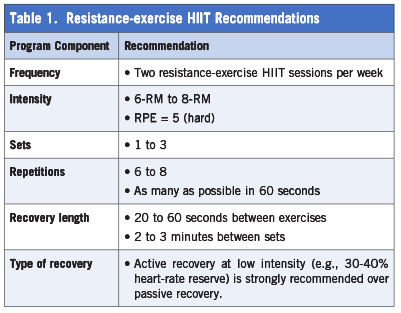
Clients should initially participate in traditional resistance training for a few months prior to engaging in resistance-exercise HIIT. Additionally, all clients should first be instructed on proper lifting technique and breathing patterns. The recommendations presented in Table 1 can be used to design an appropriate training program when a client is ready to commence with resistance-exercise HIIT.
References
American College of Sports Medicine (2014). ACSM’s Guidelines for Exercise Testing and Prescription (9th edition). Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins.
Francois, M.E. et al. (2016). Resistance-based interval exercise acutely improves endothelial function in type 2 diabetes. American Journal of Physiology: Heart and Circulatory Physiology, 311, H1258-H1267.
Francois, M.E. et al. (2014). ‘Exercise snacks’ before meals: A novel strategy to improve glycaemic control in individuals with insulin resistance. Diabetologia, 57, 1437-1445.
Giessing, J. et al. (2016). A comparison of low volume ‘high-intensity-training’ and high volume traditional resistance training methods on muscular performance, body composition, and subjective assessments of training. Biology of Sport, 33, 241-249.
Kessler, H.S., Sisson, S.B. and Short, K.R. (2012). The potential for high-intensity interval training to reduce cardiometabolic disease risk. Sports Medicine, 42, 489-509.
Paoli, A. et al. (2012). High-intensity interval resistance training (HIRT) influences resting energy expenditure and respiratory ratio in non-dieting individuals. Journal of Translational Medicine, 10, 237.
Ramos, J.S. et al. (2015). The impact of high-intensity interval training versus moderate-intensity continuous training on vascular function: A systematic review and meta-analysis. Sports Medicine, 45, 679-692.
Rognmo, Ø. et al. (2012). Cardiovascular risk of high- versus moderate-intensity aerobic exercise in coronary heart disease patients. Circulation, 126, 1436-1440.
Weston, K.S., Wisløff, U., Coombes, J.S. (2014). High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: A systematic review and meta-analysis. British Journal of Sports Medicine, 48, 1227-1234.
Wingfield, H.L. et al. (2015). The acute effect of exercise modality and nutrition manipulations on post-exercise resting energy expenditure and respiratory exchange ratio in women: a randomized trial. Sports Medicine–Open, 1, 11.




 by
by