In an effort to help you more efficiently earn continuing education credits while you explore
CERTIFIED™, you can now take the quiz as you read. Get the latest, science-based information
while you earn 0.2 CECs.
by By Lance C. Dalleck and Angela M. Dalleck
Given its prevalence—nearly 10 million American adults—you probably know someone, or may even have clients, who have suffered a stroke. According to the American Heart Association, nearly 800,000 people experience a new or recurrent stroke each year, with the prevalence increasing with age in both females and males.
Strokes occur when the blood supply to the brain is cut off (an ischemic stroke) or when a blood vessel in the brain bursts (a hemorrhagic stroke). Like a heart attack, an ischemic stroke results from a blockage in a vessel—but instead of in the heart, it occurs in the brain. Ischemic strokes account for about 87% of all strokes and are usually caused by a fatty deposit in the lining of the vessel (atherosclerosis). Hemorrhagic stroke is caused by the rupture of a blood vessel with bleeding out into the surrounding tissue(approximately 13% of all strokes).
As a health coach or exercise professional, it’s important to understand the unique exercise-programming requirements of this vulnerable population. For example, it is common for long-term disability and depression to accompany strokes. In fact, stroke is the leading cause of serious long-term disability in American adults. Moreover, it has been reported that approximately one-third of stroke survivors are likely to develop post-stroke depression, with the frequency highest in the first year. In this article, we share insights that will help guide your work with individuals who have experienced a stroke and provide you with the information you need to create safe and effective programs for this clientele.
The Challenge of Comorbidities
Many people can survive a stroke, but rarely without some type of resulting damage, as strokes can drastically reduce a person’s quality of life, robbing them of the ability to speak or utilize facial, arm and leg muscles; they may also experience other neurological impairments. Additionally, clients who have experienced a stroke typically present in a severely deconditioned state, leading to a variety of comorbidities and significantly increasing their risk of recurrent stroke and heart attack. In fact, an estimated 75 to 99% of individuals who have had a stroke also have one or more comorbidities, such as hypertension, diabetes and cancer. Comorbidities not only increase the likelihood of developing a stroke but also worsen stroke prognosis, especially for those who are older.
Given the strong likelihood that your client will possess multiple chronic conditions, as a health and exercise professional it is important for you to be prepared to meet the challenge of developing a suitable comprehensive exercise program that addresses each of your client’s chronic conditions. Here are a few considerations:
One strategy we have used with clients with comorbidities is to work on the most limiting one first (as opposed to the most serious). This approach can unlock potentials that were not present before. For example, working on strength and posture can improve mobility, which might make it possible for the client to finish cardiorespiratory exercise sessions. This, in turn, may help them better manage comorbidities they may have, such as hypertension and type 2 diabetes. This progressive approach allows clients to experience real progress as opposed to only seeing their restrictions.
The complexity of working with clients possessing multiple chronic conditions requires a thorough preparticipation health screening and organized documentation. As such, using SOAP notes—which stands for subjective, objective, assessment and plan—can be a great solution for documenting assessments, sessions and observations. You can find more information on how to take SOAP notes in the sidebar below.
SOAP—or subjective, objective, assessment and plan—notes make it possible for you to document continuing client encounters in a structured way. As used by health and exercise professionals, content for each section of the SOAP note is defined as follows:
Subjective: Observations that include the client’s own status report, a description of symptoms, challenges with the program and progress made
Objective: Measurements taken (e.g., vital signs, height, weight, age, posture and results from exercise tests), as well as exercise and nutrition log information
Assessment: A summary of the client’s current status based on the subjective and objective observations and measurements
Plan:A description of the next steps in the program based on the assessment
The wording in each section of the SOAP note should concisely and accurately document all discussions and activities, and it is essential that you date every SOAP note. This is an elegant and efficient way to document both what the client communicates and feels and what you hear and observe. Over time, SOAP notes can be a useful tool to provide feedback to the client. On that point, we have also used SOAP notes in conjunction with the ACE Mover Method to facilitate healthy lifestyle behavior change.
Understand the Effects of Common Medications
The medical management of stroke can include a broad range of medications. Also, as mentioned in the previous section, individuals who experience a stroke commonly have various comorbidities, such as hypertension and type 2 diabetes. Therefore, it is critical that you understand the interaction of certain medications with the exercise response and how your client’s exercise program might need to be adjusted. For example, the most important modifiable risk factor for stroke is hypertension, and beta blockers and ACE inhibitors are among the most common medications prescribed to Americans to manage hypertension.
Beta blockers function by preventing the binding of epinephrine to receptors in the heart. This results in decreased resting and exercise heart rates, as well as lower blood pressure values. The therapeutic effect provided by beta blockers also creates an altered physiological response to exercise. Beta blocker treatment blunts the usual increases in heart rate and blood pressure that correspond to higher exercise intensities and workloads. The fact that beta blockers attenuate the heart-rate response to exercise means traditional methods for establishing target heart rate (e.g., peak heart rate method or heart-rate reserve method) are likely to be invalid. Therefore, the most important program design modification for clients taking a beta blocker is to use an alternative method for setting target intensity. The talk test is an excellent option.
ACE inhibitors (or angiotensin-converting enzyme inhibitors) are another category of medication primarily used for the treatment of hypertension. Individuals using ACE inhibitor medication have lower resting and exercise blood-pressure values. A primary concern for clients taking ACE inhibitors is that the combination of the reduction in blood pressure from the medication combined with a natural-occurring post-exercise hypotension can result in excessive reductions in blood pressure. An easy solution is to add two to three minutes of cool-down after every exercise.
Exercise Programming Considerations
Rehabilitation following stroke typically focuses on optimizing basic activities of daily living skills: regaining balance, coordination and functional independence, and preventing complications and stroke reoccurrence. Unfortunately, this low level of rehabilitation does not provide a sufficient cardiorespiratory exercise stimulus needed to reverse the physical deconditioning, muscular atrophy, and increased cardiovascular risk resulting from stroke and associated neurological impairment. However, research has shown that individuals can improve their functional capacity through a range of exercise modalities, such as bicycle ergometer exercise, water exercise and weight-supported treadmill exercise, as well as gait, balance and coordination activities.
For many years, clinicians considered the window for motor improvement after a stroke to be within the first three to six months. However, there is evidence showing that exercise can improve selected motor performance even years after a stroke. Therefore, people recovering from a stroke may gain additional benefit and improved quality of life by working with a health and exercise professional following their release from a clinical rehabilitation program. Ideally, program guidelines should come from the physical and/or occupational therapist overseeing the clinical course of rehabilitation.
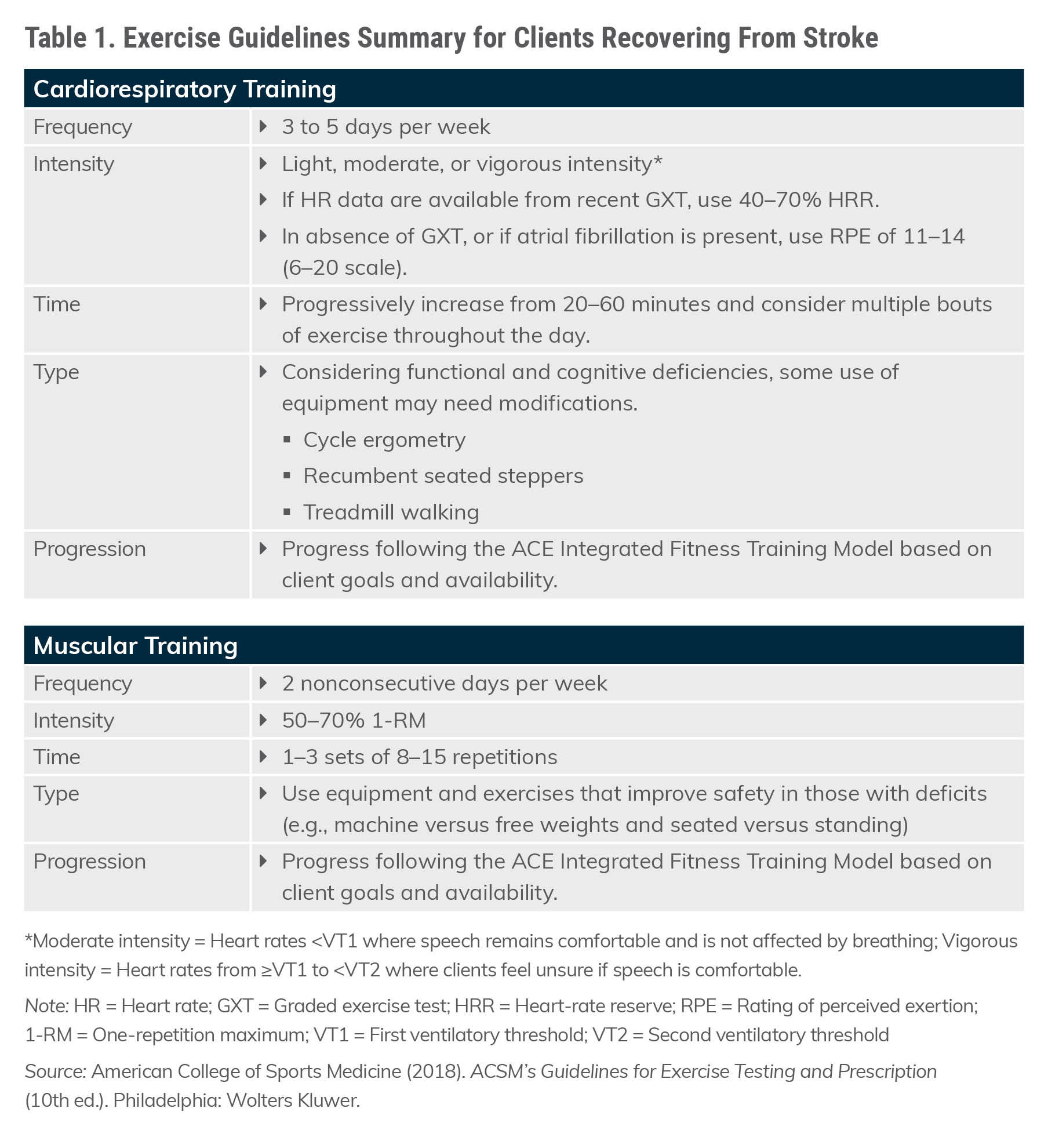
Clients who are at risk for, or have experienced, a stroke should follow the same guidelines used for heart disease and hypertension. Exercise activities may vary depending on the client’s neurologic deficit profile, current functional capacity and risk-factor status. Modalities such as using a cycle ergometer, walking/treadmill training, water exercise and other exercise classes can be modified to accommodate clients who have survived stroke. Activities that improve balance and coordination can be helpful.
The exercise guidelines presented in Table 1 can be used for cardiorespiratory and muscular training with your clients who have experienced a stroke.
Monitor Clients Closely
The wide-ranging symptoms following a stroke mean your clients require careful supervision during their exercise sessions. The brain controls various body functions, so symptoms of a stroke vary according to what area of the brain has been affected. Typical effects of a stroke include facial droop, weakness or paralysis of the body, vision problems, memory loss, and speech or language problems.
It is essential to be aware of the warning signs of a stroke:
Sudden numbness or weakness of the face, arms or legs
Sudden confusion or trouble speaking or understanding others
Sudden trouble seeing in one or both eyes
Sudden walking problems, dizziness, or loss of balance and coordination
Sudden severe headache with no known cause
Additionally, the simple acronym FAST (facial drooping, arm weakness, speech difficulties and time to call emergency services) serves as a useful mnemonic to help you recognize and respond to the needs of a client having a stroke.
A difficult reality for many who experience a stroke is a decline in cognitive function. Accordingly, additional supervision is warranted to ensure individual exercises and the overall exercise program are being performed correctly and safely.
Summary
Working with clients who are recovering from a stroke can be challenging, yet highly rewarding. By understanding the condition and the impact that certain medications may have on exercise response, thoughtfully managing comorbidities and careful exercising programming, you can play a major role in improving the health of your clients by helping them be more active and positively modifying their lifestyle risk factors.
Sign up to receive CERTIFIED™
CERTIFIED™ is a free online monthly publication from ACE designed to equip certified fitness professionals and health professionals alike with the knowledge they need to continue growing.
Author
Lance C. Dalleck, PhD
Contributor
Lance C. Dalleck, PhD, is a professor of Exercise and Sport Science at Western Colorado University. His research interests include improving exercise performance and health outcomes through evidence-based practice, quantifying the energy expenditure of outdoor and non-traditional types of physical activity, and studying historical perspectives in health, fitness and exercise physiology. Dr. Dalleck is a member of the ACE Scientific Advisory Panel.
In an effort to help you more efficiently earn continuing education credits while you explore
CERTIFIED™, you can now take the quiz as you read. Get the latest, science-based information
while you earn 0.2 CECs.
Sign up to receive CERTIFIED™
CERTIFIED™ is a free online monthly publication from ACE designed to equip certified fitness professionals and health professionals alike with the knowledge they need to continue growing.