



 by
by Do you tell your clients to “squeeze those glutes” or “tighten that core” during the execution of an exercise? These cueing techniques are spoken everywhere from physical therapy clinics to high-performance facilities across the globe. Presumably, the goal is to ensure that the participant is appropriately using the target movers and/or stabilizers for the task at hand. Of course, not all cues are appropriate for every exercise or help the client achieve the maximum benefit of any given exercise.
The execution of any movement is the sum of some incredible processing and coordination of motor signals to the musculoskeletal system and the ongoing feedback from peripheral sensory receptors as well as visual, vestibular and auditory input. For competency, efficiency, safety and maximum benefit, exercise professionals and health coaches may provide verbal, visual and sometimes tactical cues to the client with respect to movement execution.
For example, your client performs a plank and you cue him or her to keep the core tight. In another example, your client does a wood-chop movement using a cable machine and you may use the exact same cue. It is clear that both of these exercises have very different biomechanical and neurological characteristics to them. The plank is a statically held exercise that directly places the core in a loaded position as gravity acts perpendicularly to the torso’s position. The wood chop is a dynamic movement, with the body orientated vertically and with movement through multiple planes, which requires coordination and timing of the muscular force production.
Is the desired outcome of the cue the same for both exercises? The answer is no. Although the core may be involved in both exercises, the purpose of the exercise, the role of the core and your expectation of the client are all very different. If this is the case, will the client be able to differentiate between what is implied and what is said?
A better approach is to urge your clients to utilize a technique called focus of attention. From a motor skill-learning perspective, this term can be de?ned as “the conscious effort of an individual to focus their attention through explicit thoughts in an effort to execute a motor skill with superior performance” (Benz et al., 2016).
Focus of attention can be broken down to intrinsic focus of attention (IFA) and extrinsic focus of attention (EFA). Intrinsic focus is attention to parts of the individual’s body (glutes, core, knee, spine, etc.). The client is being asked to execute a movement based on what part or parts of the body he or she is consciously controlling with greater attention than other parts of the body. Extrinsic focus refers to targets outside the body and can be related to distance, direction and analogies (e.g., “keep your shoulder over your hips,” “get long,” and “open up like a book”).
Here’s another way to consider these two concepts: While IFA could be described as highlighting the “players” and strategies of the movement, EFA might be described more an external objective of the movement.
The terms motor learning and motor control are sometimes used interchangeably, yet they are different. Motor control refers to how the nervous system directs the muscles and joints to perform an action. Motor learning refers more to the acquisition of a new movement skill that remains after the practice session(s).
A strong body of research supports the use of EFA to enhance motor learning in more complex movements (e.g., wood chops, lunges, sport specific techniques). This is because the movement requires limited conscious thought and becomes more unconscious and automatic with a reflex mode of control (Wulf et al., 2010).
Conversely, IFA increases self-awareness and leads to self-regulating adjustments, which would interfere with coordinated movements in more complex movements. I often refer to this scenario with my clients as “getting in our own way,” as we ascend their corrective programs to include more integrated movements.
Returning to the wood-chop example, if you are instructing your client to keep his or her core tight, yet those same muscles are supposed to be contributing to the motion, a movement conflict may arise. If the abs are overly tightened and braced, how do they efficiently eccentrically load at the top of the movement? And then how do they maximally concentrically contract by the end of the movement?
Biomechanically, you can’t do both at the same time and optimize the muscle synergy and timing necessary for coordinated movement. Will the core tighten during the course of the movement? Yes, but the contraction force of the core muscles should not be held constant through the movement while being dictated by higher levels in the brain. This is contrary to the movement sequence being more unconscious and automatic with a reflex mode of control.
When working with clients with chronic pain at Function First, I use the metaphor of a volume knob for how much force our muscles produce during movement. The volume knob on zero would be a neurologically “silent” muscle, while the volume knob at 10 would be considered a maximum contraction. Movement should see a fluctuation of the volume going up and down based not only on the task at hand, but also during different phases of that task. Coaching the client to turn his or her core up to an 8 on the volume knob, and to keep it there throughout the movement, interferes with the authenticity of the motion and does not allow for the necessary variability of strength of contraction through the movement.
The previously mentioned limitations of IFA, which were described as disadvantages for complex movements, can, in fact, be advantageous for lower-level corrective exercises, especially when working with clients in pain. Spatial and proprioceptive acuity is diminished in those with chronic pain. Therefore, using an IFA strategy with isometric contractions and or isolated movements can increase the corticospinal excitability (motor neuron activity from the brain and spinal cord) of the associated muscle groups. This can assist the client in regaining awareness and strength of targeted muscle groups and ultimately their contribution to more involved movements.
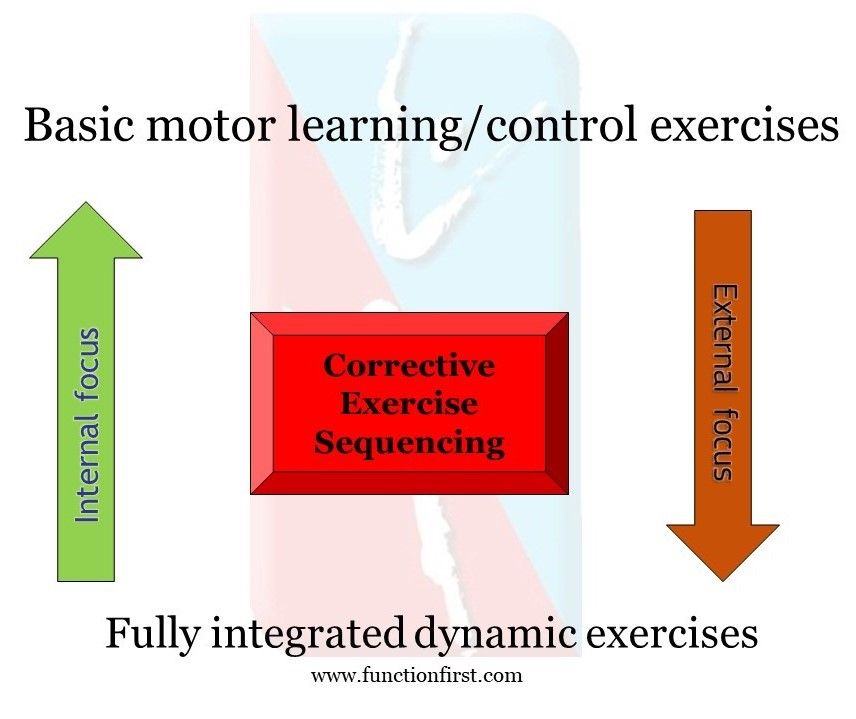
The image below represents principles that we apply as Pain-free Movement Specialists when designing corrective exercise programs for clients in pain. The image summarizes an inverse relationship between IFA and EFA and the types of exercises that might map best to these principles.
A final point to consider when determining the cues you give to your clients is the resulting change in the arthrokinematics of the joint. Arthrokinematics describes the motion between joint surfaces. This motion is determined by the shapes of the two joint surfaces and the timing and the force of the muscle contractions acting on the joint and external forces (e.g., gravity).
For example, during a side lateral dumbbell raise, you cue your client to squeeze the shoulder blades together and not to let them go while the arm is raised. The intention, of course, is to maintain good posture and positioning of the scapula in the frontal plane, but by limiting the ability of the scapula to upwardly rotate at the end of the movement, the arthrokinematics have been changed.
This has a potential negative consequence, as it may increase mechanical stress on the soft tissue around the joint and increase compression of the joint surfaces.
Both internal focus of attention (IFA) and external focus of attention (EFA) cueing offer benefits when applied at the optimal time and for the appropriate exercises or movements. IFA can help clients with chronic pain or those who are deconditioned or in post-rehab improve awareness and recruitment of poorly functioning muscles or muscle groups. When cueing for more involved movements requiring greater motor control, EFA allows the client to focus on the outside objective, creating more efficient movement and reflexive error correction.
With clients who have chronic pain, we use both cueing approaches within a given session as the programming ascends from remedial/floor-based exercises to more vertical and integrated movements. This moves the client through a continuum of what we call “sub routines” or programs within a program that best elicits the motor control needed to build movement confidence.
References
Benz, A. et al. (2016). Coaching instructions and cues for enhancing sprint performance. Strength and Conditioning Journal, 38, 1–11.
Wulf, G., Shea, C. and Lewthwaite, R. (2010). Motor skill learning and performance: A review of influential factors. Medical Education, 44, 75–84.



 by
by