
BY LANCE DALLEK, Ph.D.
Fall incidence rates currently pose a serious health problem for older adults. Among those who are 65 or older, it has been estimated that 35 percent to 45 percent of otherwise healthy, community-dwelling adults fall at least once a year.
Decreased balance is attributable to an age-related decline in multiple physiological systems that contributes to decreased muscle flexibility and strength, reduced central processing of sensory information, and slowed motor responses (American Geriatrics Society, British Geriatrics Society, and American Academy of Orthopedic Surgeon Panel on Falls Prevention, 2001). In addition to an increased risk of falls, diminished balance and mobility may limit activities of daily living or participation in leisure-time activities. Accordingly, it is essential that balance exercises be incorporated into the physical activity programs of older adults. The following article uses case studies to outline the critical components of designing individualized balance exercise programs for clients that reduce their risk of falls. Sample balance exercises and training progressions (from simple to complex) will also be presented.
Origin of Poor Balance and Falls
An understanding and knowledge of the factors contributing to impairments in balance is fundamental to designing an effective balance-training program. Poor balance is multi-factorial in origin; in particular, cognitive impairment, visual disturbances and poor reaction time increase the likelihood of falls. Moreover, balance impairments and lower-extremity skeletal muscle weakness are also well-recognized independent contributors to falls. In particular, fallers have less muscular strength in the quadriceps and ankle dorsiflexors and plantarflexors compared to non-fallers (Orr et al., 2008). It should be noted, however, that previous research exploring exercise training as a means for fall prevention in older adults has shown conflicting results (Mansfield et al., 2007). While some studies have reported a reduced risk of falls after exercise training, other research has reported limited or no benefits. Even so, there are important lessons to be learned from these incompatible findings, and the complex etiology of poor balance highlights the need for a comprehensive intervention program. With that in mind, consider the following six critical issues that must be considered when developing an all-inclusive strategy for optimizing balance training and fall prevention among older clients.
1. Multi-component training is superior to single-component balance training.
The explanations generally given for lack of a favorable adaptation from balance exercises are 1) lack of specificity with training, and 2) performance of single-component compared to multi-component training. It has been reported that training programs including only single-task activities fail to place the client in an environmental condition similar to that experienced prior to and during a fall (Silsupadol et al., 2009). Importantly, though balance training focused on improving functional tasks (e.g., heel-toe walking or standing on one leg) will be successful for enhancing performance of that specific activity, it fails to adequately replicate activities of daily living that require maintaining balance while completing several activities simultaneously or while distracted. A well-designed exercise program should feature concurrent performance of balance exercises and additional tasks. For example, in addition to performing heel-toe walking, the client may simultaneously be asked to complete a cognitive task, such as counting backward from 100 by increments of three. An additional form of dual-component training may involve combining a balance exercise with another form of physical activity. For instance, the client could be asked to balance on one leg while playing catch with a light medicine ball. In summary, multi-task balance training more closely replicates the activities of daily living in which a client’s balance performance is most likely to be challenged by a disturbance.
2. Simulate loss of balance during training.
Balance-training programs and fall-prevention interventions must include a focus on balance-recovery reactions (Mansfield et al., 2007). Ultimately it is the capability—or lack thereof—to recover from a balance perturbation (loss of balance) that eventually determines whether or not a client falls. Balance disturbances can arise from collisions, slips and trips. Additionally, loss of balance can occur during voluntary movements, including bending, reaching and turning. Our body has a natural line of defense against balance disturbances: rapid limb movements. For example, reaching out to grab a supporting object or quickly stepping forward with a lower limb are compensatory mechanisms aimed at preventing a fall. Accordingly, it is logical to address the balance-recovery skill levels of clients because effective training programs will be those that replicate sudden and unpredictable balance disturbances. Importantly, to elicit the most favorable adaptations in a client’s balance-recovery reaction capacity, the exercises and activities should be designed in a way that does not permit the client to anticipate a balance perturbation.
3. Couple resistance training with balance training.
Despite the fact that poor balance is frequently associated with reduced muscular strength, the literature does not currently support resistance training alone as a successful strategy for enhancing balance performance and fall reduction. A systematic review of the efficacy of resistance training as an isolated intervention for uniformly improving balance revealed that this approach was successful in only one of five instances (Orr et al., 2008). Therefore, it is crucial to remember that resistance training needs to also be coupled with balance training for positive modifications to be conferred on postural stability. Indeed, the integrated exercise-training approach has been found to be effective in the literature (de Bruin and Murer, 2007).
4. Correctly sequence balance exercises.
Aerobic, resistance, flexibility and balance training are each critically important for the overall health, functional capacity and quality of life of older adults. However, to fulfill the minimum frequency requirements of each form of activity, clients will need to perform at least two (or more) activities on the same day, and most likely within the same exercise session (Nelson et al., 2007). Research has reported that participation in either resistance or flexibility activities prior to balance exercise can negatively impact performance (Behm et al. 2004; Moreland et al. 2004), so balance training should precede both resistance and flexibility activities. For the senior client who may already face significant balance challenges, it would be inappropriate (and possibly harmful) to create additional perturbations due to improper activity sequencing. Balance training (when combined with resistance and flexibility activities) should be performed first or following aerobic activity.
 5. Create innovative balance exercises.
5. Create innovative balance exercises.
Conventional balance-training programs include various sitting and standing activities, which, for the motivated client, has been shown to be effective over the long-term. However, in less-motivated individuals the performance of repetitive, basic tasks can lead to poor adherence, less-effective training and ultimately cessation of training. Consequently, continuously designing novel and creative balance exercises for clients is essential. Recent research has reported that utilizing interactive video games may be an effective strategy to employ with designing balance activities for older adults (Nitz et al., 2009). For example, the Wii Fit has various balance modules, including soccer, skiing and penguin, which can be performed at different skill levels, depending on the client’s functional capacity. Science has shown that progressively incorporating interactive video games into training can increase motivation and improve balance performance (Betker et al., 2006).
6. Change the availability of sensory cues.
Many falls occur during conditions that are unfamiliar to the client. Poor lighting or uneven surfaces impair the sensory cues typically available, therefore temporarily compromising the balance performance. These challenges can be introduced into the training program as a means to better prepare clients for circumstances where sensory cues are unavailable (Silsupadol et al., 2009). For instance, the client might perform heel-toe walking while wearing sunglasses (inside), with eyes closed, or while slowly turning the head from side-to-side. Additionally, standing balance exercises can be completed while standing on a foam pad or balance disk in an effort to disturb the surface conditions. Regardless of which techniques are utilized, altering the sensory cues available to a client is an important consideration when preparing the overall balance-training program.
F.I.T.T. Recommendations for Balance Training
The frequency, intensity, time and type (F.I.T.T.) approach to exercise program design can also generally be applied to balance-exercise programming (ACSM, 2010). Although research has yet to identify the optimal frequency, intensity, duration and type of balance exercises, it has been recommended that balance training be performed for 10 to 15 minutes, three days per week (Nelson et al., 2007), and the intensity should be safe, but challenging. Balance training should be integrated into the overall physical activity program according to the sequencing guidelines discussed earlier.
Effectively Progressing Balance-training Exercises
A program designed to optimize balance training and fall reduction and prevention should incorporate each of the key points discussed earlier. Clients with no previous balance-training experience should initially perform basic sitting and standing exercises as a means to improve balance performance. As these initial exercises become easier, an increase in difficulty can be accomplished in numerous ways (ACSM, 2010):
1. Arm progressions: Vary the use and position of the arms to make a given balance exercise more difficult. Initially, the client may need to grasp or touch another object, such as a wall or back of a chair, to facilitate balance. Progressively, exercises can be performed with arms spread out and raised to shoulder height to assist with stability. Ultimately, clients can move arms in from sides to a folded position across the chest.
2. Surface progressions: Alter the surface or apparatus on which clients perform balance exercises, progressively increasing the difficulty. For instance, foam pads, balance disks and BOSU balls can be substituted for a hard, flat surface while performing multiple standing balance exercises. Similarly, stability balls can be exchanged for regular chairs when performing sitting exercises.
3. Visual progressions: Try mitigating the visual sensory cues provided to the client during balance exercises. For example, the lighting of the room can be gradually dimmed, sunglasses may be worn inside, or eyes may be shut completely.
4. Tasking progressions: Require clients to initially master each balance exercise performed as a singular task. When this level of achievement is attained, additional tasks should be supplemented to the routine. Cognitive tasks or added physical tasks are a few of the readily available options.
In addition to gradually increasing the difficulty of a balance exercise, it is paramount to continuously seek novel and fun balance exercises for clients. While many clients will want to seek greater challenges, they should be cautioned about proceeding in difficulty without first demonstrating competency at the current level of balance exercise. After all, progressing too rapidly can actually contribute to a fall. Refer to Table 1 and Figures 1a–c, which feature sample balance exercises and a training progression (from simple to complex).
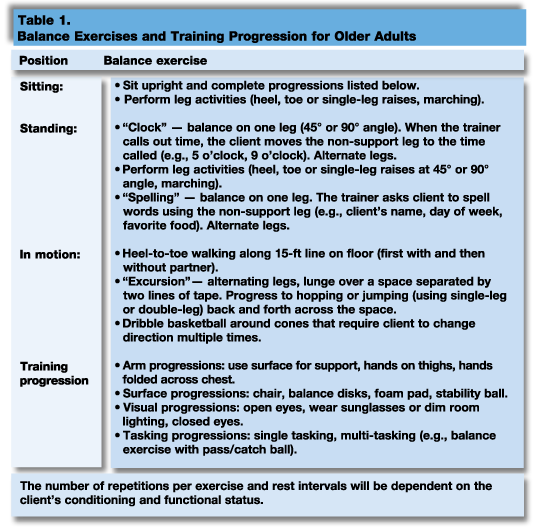

Figure 1a.
Sample progression of sitting balance exercises (closed eyes, arms crossed, stability ball)
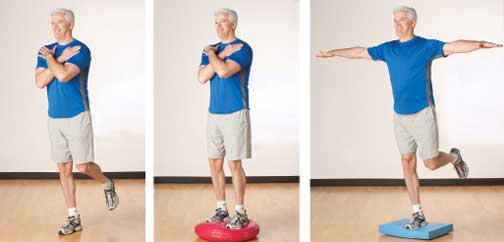
Figure 1b.
Sample progression of standing balance exercises (single-leg stable surface, unstable surface, single-leg unstable surface)

Figure 1c.
Sample progression of in-rotation balance exercises (heel-to-toe, excursion, multi-tasking)

Download a PDF of a Case Study Approach to Balance Training.
References
American College of Sports Medicine. (2010). Resources for the Personal Trainer, 3rd ed. Baltimore: Lippincott Williams & Wilkins.
American Geriatrics Society, British Geriatrics Society and American Academy of Orthopedic Surgeon Panel on Falls Prevention. (2001). Guideline for the prevention of falls. Journal of the American Geriatrics Society, 49, 5, 664–672.
Behm, D.G., Bambury, A., Cahill, F. and Power, K. (2004). Effect of acute static stretching on force, balance, reaction time and movement time. Medicine & Science in Sports & Exercise, 36, 8, 1397–1402.
Betker, A.L., Szturm, T., Moussavi, Z.K. and Nett, C. (2006). Video game-based exercises for balance rehabilitation: A single-subject design. Archives of Physical Medicine & Rehabilitation, 87, 8, 1141–1149.
de Bruin, E.D. and Murer, K. (2007). Effect of additional functional exercises on balance in elderly people. Clinical Rehabilitation, 21, 2, 112–121.
Mansfield, A., Peters, A.L., Liu, B.A. and Maki, B.E. (2007). A perturbation-based balance training program for older adults: Study protocol for a randomized controlled trial. BMC Geriatrics, 7, 12.
Moreland, J.D., Richardson, J.A., Goldsmith C.H. and Clase, C.M. (2004). Muscle weakness and falls in older adults: a systematic review and meta-analysis. Journal of the American Geriatrics Society, 52, 7, 1121–1129.
Nelson, M.E., et al. (2007). Physical activity and public health in older adults: Recommendation for adults from the American College of Sports Medicine and the American Heart Association. Medicine & Science in Sports & Exercise, 39, 8, 1435–1445
Nitz, J.C., Kuys, S., Isles, R. and Fu, S. (2009). Is the Wii Fit a new-generation tool for improving balance, health and well-being? A pilot study. Climacteric, Nov 12.
Orr, R., Raymond, J. and Singh, M.F. (2008). Efficacy of progressive resistance training on balance performance in older adults: A systematic review of randomized controlled trials. Sports Medicine, 38, 4, 317–343.
Silsupadol, P., et al. (2009). Effects of single-task versus dual-task training on balance performance in older adults: A double-blind, randomized controlled trial. Archives of Physical Medicine & Rehabilitation, 90, 3, 381–387.
______________________________________________________________________
Lance C. Dalleck, Ph.D., is coordinator of the Cardiac Rehabilitation/Clinical Exercise Physiology graduate program at Minnesota State University, Mankato. His research interests include improving exercise performance and health outcomes through evidence-based practice, quantifying the energy expenditure of outdoor and non-traditional types of physical activity, and studying historical perspectives in health, fitness and exercise physiology.