
By FABIO COMANA, M.A., M.S.
With the passage of Title IX in 1972, competitive sports for girls and women in the U.S. changed forever. In fact, from 1972 to 2006, the number of females participating in high school sports grew from 300,000 to an estimated 3 million, an increase of almost 1,000 percent (Lal and Hoch, 2007; Giugliano and Solomon, 2007). Greater participation in sports by females has also heightened awareness of the health and medical issues specific to the female athlete. In particular is the knee joint, the site of the highest injury rates among female athletes (Parkkari et al., 2008). Studies comparing female athletes' susceptibility to injury of the anterior cruciate ligament (ACL) have shown that women have considerably higher rates of injury, suffering ACL tears at a four- to six-times greater rate than male counterparts in the same sport (Myer et al. 2008). Statistics suggest that each year one in every 10 college female athletes and one in every 100 high school female athletes will sustain a serious knee injury.
Approximately 70 percent of ACL injuries are non-contact in nature, occurring in sports that involve jumping and landing, quick stopping, cutting and directional changes. Although the ACL is the most commonly injured area of the knee, injuries to the menisci, other ligaments, joint cartilage and the underlying bone structure also occur frequently (Lohmander et al., 2007). Therefore, knees injuries also should be evaluated for meniscus tears, which occur in almost 50 percent of cases.
Athletes suffering a knee injury face the prospect of losing an entire season of play; expensive surgery and a slow process of rehabilitation; emotional and cognitive setbacks that may impact overall quality of life, relationships and academics; potential scholarship losses; and the possibility for some permanent structural and functional impairment (e.g., developing arthritis within the injured knee joint) (Giugliano and Solomon, 2007; Parkkari et al., 2008). Unfortunately, even after extensive rehabilitation, ACL-injured athletes experience a higher incidence of re-injury upon return to their sport, ranging from 2 percent to 13 percent (Giugliano and Solomon, 2007).
Why Are Female Athletes More Prone to Knee Injuries?
Numerous factors contribute to the discrepancy between male and female knee injury rates (Adachi et al., 2008; Barber-Westin et al., 1997; Beynnon et al., 2006; Giugliano and Solomon, 2007; Hal & Hoch, 2007; Lohmander et al., 2007; Parkkari et al., 2008; Renstrom et al., 2008). Much of the research focuses upon the following causes:
Structural and Anatomical Differences
- Wider pelvis, coupled with shorter bones that increases the Q-angle between the quadriceps muscle on the front of the thigh and the patellar tendon.
- A narrower intercondylar or femoral notch that may cause a “shearing” effect (fraying and weakening) on the ACL by the femur during cutting and jumping movements.
- Pronation at the foot causing internal rotation of the tibia coupled with a greater degree of rotation at the femur, which increases stresses along the ACL.
- Smaller ligaments and bone surfaces for ligament attachment.
Hormonal Differences
- The ACL contains receptors for both estrogen and progesterone and some researchers suggest that increases in one or both of these hormones may loosen the ACL and heighten its potential for injury. A woman’s ligaments exhibit greater laxity during pregnancy due to changing hormonal levels, which may also explain why the risks for injury may vary within the menstrual cycle (e.g., higher during the ovulatory phase of the menstrual cycle).
- The use of oral contraceptives, which alter hormonal levels of estrogen.
- Estrogen directly and indirectly affects the female neuromuscular system and may alter neuromuscular response activity.
Gender, Skill and Training Differences
- Lower neuromuscular coordination when compared to males. Boys have historically begun training at a younger age, facilitating earlier development of footwork, eye-hand coordination, and catching and throwing skills, all of which develop the neuromuscular system. Girls often miss this early exposure to motor learning, placing them at a distinct disadvantage when they become involved in high school sports. Consequently, females generally demonstrate lower abilities and skills, inferior technique and often receive less coaching, all of which contribute to a higher incidence of knee injuries.
- Inadequate strength and slower muscle-reaction times.
- Landing biomechanics and muscle utilization patterns. Males demonstrate relatively higher involvement of the hamstrings and gastrocnemius during jump-landing, while females favor quadriceps action to control anterior tibial translation, especially during the first 40 degrees of knee flexion. The hamstrings are an ACL agonist, lengthening eccentrically during this hip-flexion/knee-flexion phase. This reduces the strain placed upon the ACL as they help hold the tibia close to the femur, controlling or minimizing anterior tibial translation. To demonstrate this point, place your hands over your hamstrings and perform both a quad-dominant and glute-dominant squat, noticing the difference in hamstrings tension. During the glute-dominant squat you should notice increased tension in the hamstrings indicating an eccentric load that helps unload the ACL. Quadriceps contraction during this phase of knee flexion (where injury most often occurs) increases strain upon the ACL due to increased shearing forces as the quadriceps attempt to control anterior tibial translation.
First Step to Reducing Injuries: Increase Stability and Mobility
Regardless of the contributing factors, skill- and conditioning-level or movement technique, when females are exposed to a potential injury situation (e.g., being off-balance, sudden stops or twisting), they may lack adequate strength, coordination and reactivity to avoid injury. Sufficient muscle strength, coordination, balance, reactivity and good technique can potentially spare the athlete from injury. To improve chances of protecting the knee, coaches and trainers need to instruct good technique, and develop hamstrings strength and reactivity, balance (proprioceptive function), core conditioning and agility, and improve movement efficiency when performing the primary movements of the lower extremity. We can essentially divide our daily activities into two primary movements: the bend-and-lift pattern (squat, dead lift) and single-leg patterns (single-leg stance, step, lunge). A consistent theme with all coaches and trainers working with athletes is the need to train these movement patterns as a pre-requisite to instructing and implementing exercises. Being able to perform these primary movements effectively while also possessing appropriate levels of stability and mobility throughout the kinetic chain, will improve an individual’s potential for efficient movement and decrease the likelihood for compensation, pain or injury (Cook and Jones, 2007; Gray and Tiberio, 2007).
To create an effective preventative program for female athletes, trainers and coaches must consider the following factors (Cook and Jones, 2007; Giugliano and Solomon, 2007; Gray and Tiberio, 2007; Lal and Hoch, 2007; Parkkari et al., 2008; Renstrom et al., 2008):
- Awareness of the anatomical and physiological differences between males and females, including potential hormonal effects
- Sport demands, prevalent injuries and previous injuries of the athlete
- Overall athleticism (skills, conditioning and abilities) of the athlete
- Pre-participation evaluations to identify underlying weaknesses (side-dominance), movement compensations and pathological problems of the knee joint
- Appropriate exercise and drills for muscle strengthening and for improving balance, agility, coordination and reactivity. This includes the selection of appropriate exercises, drills and progressions to enhance the neuromuscular pathways to stabilize the knee (Figure 1).
- Ability to instruct proper movement mechanics for the primary movements as a foundation to more specific patterns (Figure 1).
- Training and game environment
- Complete treatment and rehabilitation of underlying pathologies prior to participation
- Adequate rest and recovery, and avoiding potential overuse
Figure 1. Planning and Programming Sequence for Developing a Preventative Program against Knee Injuries
A Well-designed Training Program is Key to Preventing Injuries
Sportsmetrics™, a three-phase program to reduce the incidence of female knee injures, was developed from research collected at the Cincinnati Sportsmedicine Research and Education Foundation. Researchers noted weaknesses, neuromuscular deficiencies and imbalances between hamstrings and quadriceps muscle strength in many female athletes (Lindenfeld et al., 1994; Hewett et al., 1996). They designed a six-week (3x /week, 60–90 minute sessions) strengthening, stretching and plyometric training program for female athletes utilizing a three-phase model (technique, fundamentals and performance phases). Results from their research demonstrated that untrained females experienced injury rates 3.6 times higher than those of the trained group and, more importantly, injury rates in the trained females were not significantly higher than in male controls. While 10 of 463 untrained female athletes sustained serious knee injuries, only two of the 366 strength-trained female athletes experienced knee problems (Lindenfeld et al., 1994; Hewett, et al., 1996). Overall improvements in the trained group demonstrated the following (Lindenfeld et al., 1994; Hewett et al., 1996, Noyes et al., 2005):
- Improved static and dynamic balance
- Improved leg strength and power (hamstring/quadriceps peak-power ratio), and neuromuscular reactivity
- Improved hamstrings-to-quadriceps strength balance and dominant- vs. non-dominant-leg hamstrings strength
- Limb symmetry equivalent to that of male athletes the same age
- Decreased knee landing forces (jump landing mechanics changed from stiff-legged and wobbly to stable and more controlled)
- Improved performance (jump height)
To better understand how to re-establish stability and mobility within the kinetic chain, it is important to have a thorough knowledge of the body’s individual joints and their relationship with one another. While the body is one integrated unit and should always be viewed as such, for the purposes of this article we will focus our attention upon the lower extremity. Here we find an interesting, yet harmonious, relationship between the foot, ankle, knee and hips (Figure 2). The foot is generally a stable joint, offering a firm platform from which to push off, while the ankle is generally more mobile, offering approximately 15–20° of dorsiflexion, 45–50° of plantar-flexion, 10–20° of inversion/eversion, and some rotation. Likewise, while the knee is primarily stable, moving mainly in the sagittal plane, the hips are a mobile joint, allowing 100–135° of flexion, 10–15° of extension, 30–50° of adduction/abduction and 30–60° of internal/external rotation (Kendall et al., 2005; Sahrmann, 2002).
During gait, the foot does relinquish some stability for mobility to absorb impacting forces as the foot accepts the load of the body and the tibia transitions forward. During this load-response instant, the foot moves into pronation and the calcaneus everts, increasing mobility within the tarso-metatarsal joints. The foot moves back into supination and the calcaneus inverts during the heel-off and toe-off instants, increasing rigidity and stability, and offering a firmer platform to push off against the ground (Gray and Tiberio, 2007).

Figure 2: The Symbiotic Relationship of Stability and Mobility in the Lower Extremity
Understanding Kinematics to Improve Movement Efficiency
To help your clients and athletes move more efficiently, it also is important to understand certain kinematics within the body, such as the important kinematic relationship that exists between the ankle, knee and hip. As discussed, during the heel strike instant of gait, reactive forces originating from the ankle dissipate forces upward through the knee and beyond; to help absorb these forces, the foot moves into pronation. As Figure 3 illustrates, pronation forces internal rotation of the tibia, which in turn drives the femur into a greater and faster degree of internal rotation (Gray and Tiberio, 2007). Assuming no structural abnormalities exist in the ankle, tibial and femoral design, the different degrees of internal rotation between the femur and tibia places stresses on the medial surface of the knee and forces the knee into abduction (valgus stress). This increases the strain placed upon the anterior cruciate ligament (ACL) ligament given its orientation (connecting from a posterior-lateral part of the femur to an anterior-medial part of the tibia). To help demonstrate this point, perform a basic movement pattern: Stand comfortably with your bare feet hip-width apart and place the palms of your hands on the fronts of your upper thighs. Slowly pronate and supinate your ankles and observe how both the tibia and femur rotate during the ankle movements.
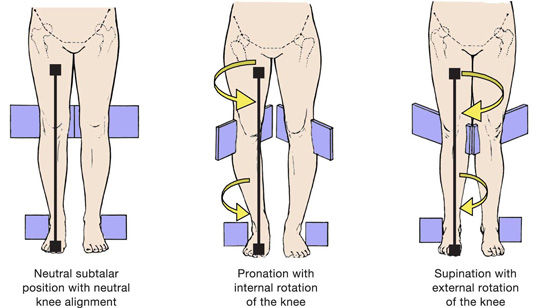
Figure 3. Ankle Pronation and Supination and the Effects Up the Kinetic Chain
Normal structural design and function of the lower extremity resists this stress with a large medial collateral ligament on the medial surface of the knee and a group of powerful posterior-lateral muscles (i.e., gluteals) at the hips that function to decelerate internal rotation (Kendall et al., 2005; Sahrman, 2002). To demonstrate this point, place your hands over your gluteus maximus. Repeat the supination and pronation movements discussed in the previous demonstration, noting how your gluteus maximus shuts on and off during the rotation (contracting concentrically with supination).
Therefore, during walking and running, gluteal activity is critical to decelerate the internal rotation associated with each step. Given the propensity that many individuals possess toward standing in pronation, which lengthens and weakens the gluteals, trainers and coaches must address how a lack of adequate gluteal activity in the transverse plane may fail to protect the integrity of the knee.
The gluteals also play an important role during the bend-and-lift movement in the sagittal plane. In observing this movement, individuals will exhibit either a glute-dominant or a quad-dominant movement pattern.
- Glute-dominance implies a reliance on eccentrically loading the gluteus maximus during a bend-and-lift (squat) movement. The first 10–15° of the downward phase are initiated by pushing the hips backward, creating a hip-hinge movement. In the lowered position, this maximizes the eccentric loading on the gluteus maximus, which can now generate significant force during the upward, concentric phase.
- Quad-dominance implies a reliance on eccentrically loading the quadriceps during a bend-and-lift (squat) movement. During the first 10–15° of the downward phase, shearing forces increase across the knee as the quadriceps try to control anterior tibial translation (Wilthrow et al., 2005). In the lowered position, the gluteus maximus is not eccentrically loaded and therefore cannot contribute significantly to the upward phase.
Another important biomechanical consideration exists with weight transference onto the stance-leg during gait. As the body moves to accept weight onto one leg, this requires a weight shift over the stance-leg while preserving optimal alignment between the hip, knee and foot. This weight transference normally involves a 1- to 2-inch lateral shift of the hips over the stance-leg coupled with a small change in hip angle, tilting that side upward by approximately 4–5° (called hip adduction) (Whiting and Rugg, 2006). Excessive hip adduction exacerbates the stresses placed upon the knee, potentially increasing the Q-angle, which enhances the possibility of a knee injury. It is the collaborative actions of the gluteal group on the stance-side (working in the frontal plane to control hip adduction) and the opposite quadratus lumborum (functioning to prevent excessive hip drop by holding the opposite hip up) that protect help the knee. Any weaknesses in these muscle groups may increase the probability of a knee injury.
Bend-and-lift Patterns
Although the bend-and-lift movement associated with the squat is arguably one of the most prevalent activities used in strength training and throughout our activities of daily living, it is subject to much controversy given its potential for harm to the knees and low back. Faulty movement patterns associated with poor technique will disrupt muscle function and joint loading, compromising performance and ultimately leading to overload and potential injury (Kendall et al., 2005, Sahrmann, 2002). Therefore, proper technique is the key differentiator. One limiting factor to good technique is a lack of ankle mobility, which according to Kendall is normally between 15° and 20° of ankle dorsi-flexion. To evaluate this limitation, have your client place one foot on a low riser (< 12”), positioning the tibia perpendicular to the floor. Next, ask them to lean slowly forward, dorsi-flexing the ankle until the heel lifts off the floor or the ankle falls into pronation, then determine the number of degrees of motion achieved. Any mobility less than 15° merits improvements in flexibility prior to teaching any bend-and-lift movements.
While the hips typically exhibit between 100° and 135° of flexion, the amount of hip flexion required during a squat averages approximately 95° (Kendall et al., 2005; Hemmerich et al., 2006). Hence, it is important to shift the pelvis posteriorly during the downward phase to facilitate adequate hip flexion. The hip-hinge exercise teaches individuals how to shift their hips backward, not only to promote additional hip flexion, but also to promote glute-dominance and reduce the shearing forces across the knee joint.
During a squat movement, the inability to stabilize the lumbar spine or maintain a straight or slightly extended thoracic spine increases compressive and shear forces within the lumbar vertebrae (Broomfield, 1998; McGill, 2006). A lack of adequate thoracic spine mobility often produces movement compensations that involve increased lumbar extension (increased lordosis). A 2° increase in lumbar extension from neutral can increase compressive forces on the vertebral discs by 16 percent over maintaining a neutral spine (Walsh et al., 2007).
During the decent phase of a bend-and-lift movement, the majority of the body’s mass is positioned behind the knees. This applies a backward pull-force upon the femurs, which in turn pulls upon the anterior cruciate ligament. Although the knee is a hinge joint, the center of rotation within the joint is not truly circular given this backward pull. While glute-dominant squatting helps stabilize the knee during the downward phase, concern arises when the downward phase is uncontrolled and forces contact between the back of the calf and the hamstrings. The ballistic nature of this contact applies additional forces to the knee, placing additional strain on the ACL (Kreighbaum and Barthels, 1996).
Once the standard mechanics of the bend-and-lift are mastered, trainers and coaches should implement variations to the standard neutral-stance position (feet parallel and hip-width apart) to mimic many of the static positions athletes may find themselves in during both acceleration and deceleration (landing) phases (Gray and Tiberio, 2007). Alter foot position in all three planes, changing the loading forces along the kinetic chain, but reinforce the need for proper alignment and weight distribution between the ankle, knee and hips. Foot positions may involve any or all of the combinations of staggered- and split-stance, wide- and narrow-stance, or internally and externally rotated foot position.
Lunge Movements
Many of the same principles of the bend-and-lift movement apply to the lunge movement, which is essentially an exaggeration of the step. While a bend-and-lift is considered a static movement (static base of support), the lunge is considered dynamic (moving base of support). Athletes will often learn and master the technique of the bend-and-lift, yet fail to demonstrate proper technique during the lunge movement. Trainers and coaches need to emphasize the same instructional techniques to the lunge (e.g., glute-dominance and hip-hinging, alignment of the knee over the second toe, torso-tibial alignment), whether it is a forward, back, side or rotational lunge. One additional approach to use with the lunge is to emphasize activation of hamstrings during the upward phase to help extend the leading knee.
Likewise, once the standard mechanics of the bend-and-lift are mastered, trainers and coaches should implement variations to the standard lunge position to mimic many of the dynamic positions athletes may find themselves in during both acceleration (cutting) and deceleration (landing) phases (Gray & Tiberio, 2007). Coach athletes to move three-dimensionally as illustrated in Figure 4 with Gray’s lunge matrix by altering the position during the step, lunge/landing position (i.e., internal and external rotation), while also reinforcing the need for proper mechanics (Gray and Tiberio, 2007).
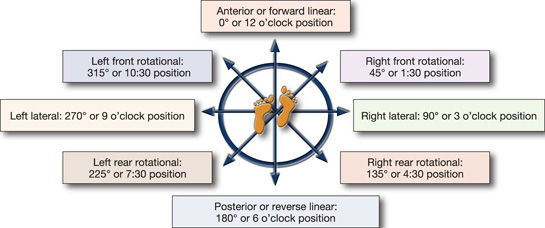
Figure 4: Directional Movements for the Lunge
Begin by initially instructing the directional movements in a pre-determined fashion as a step, then progress the drill complexity to jumps, hops or bounds. Once these movement patterns are mastered, what follows is the development of strength and fundamental skills as a pre-requisite to the implementation of plyometric drills and event-specific drills (see Figure 1). The timeframe needed to train these movements successfully depends upon individual differences, including current conditioning level, past experiences, body type, abilities and skills, attitudes, motivational levels, emotional make-up, learning style and maturation level (Schmidt and Wrisberg, 2004).
Conclusion
Reducing a client’s potential injuries—whether male or female—involves effective coaching, developing hamstrings strength and reactivity, enhancing proprioceptive function and core conditioning, and improving movement efficiency in performing bend-and-lift and single-leg patterns. Comprehension of the kinematic relationships of the lower extremity joints and re-establishing the stability-mobility relationship within the entire kinetic are critical to effective conditioning. However, because females favor quadriceps action to control anterior tibial translation during landing, re-education in favor of glute dominance with greater eccentric hamstrings loading is essential for reducing the risk of potential knee injuries.
_____________________________________________________________

Fabio Comana, M.A., M.S., is an exercise physiologist and spokesperson for the American Council on Exercise, and an adjunct professor at San Diego State University (SDSU) and the University of California San Diego (UCSD), teaching courses in exercise science and nutrition. He holds two master’s degrees, one in exercise physiology and one in nutrition, as well as certifications through ACE, ACSM, NSCA, and ISSN.
References
Adachi, N., Nawata, K., Maeta, M. and Kurozawa, Y. (2008). Relationship of the menstrual cycle phase to anterior cruciate ligament injuries in teenaged female athletes. Archives of Orthopaedic & Trauma Surgery, 128, 5, 473–478.
Barber-Westin, S., Noyes, F. and Andrews, M. (1997). A rigorous comparison between the sexes of results and complications after anterior cruciate ligament reconstruction. American Journal of Sports Medicine, 25, 4, 299–311.
Beynnon, B.D., et al. (2006). The relationship between menstrual cycle phase and anterior cruciate ligament injury: A case-control study of recreational alpine skiers. American Journal of Sports Medicine, 34, 5, 757–764.
Broomfield, J. (1998) Posture and proportionality in sport. In: Training in Sport: Applying Sport Science, Ellito, B (dE.). John Wiley & Sons, Inc.: New York, N.Y.
Cook, G. and Jones, B. (2007). Secrets of the Hip and Knee. www.functionalmovement.com
Cook, G. and Jones, B. (2007). Secrets of the Shoulder. www.functionalmovement.com
Giugliano, D.N. and Solomon, J.L. (2007). ACL tears in female athletes. Physical Medicine & Rehabilitation Clinics of North America. 18, 3, 417–438.
Gray, G and Tiberio, D (2007). Chain Reaction Function. Gray Institute Adrian, Mich..
Hemmerich, A., et al. (2006). Hip, knee and ankle kinematics of high range of motion activities of daily living. Journal of Orthopedic Research, 24, 770–781.
Hewett, T.E., Stroupe, A.L., Nance, T.A. and Noyes, F.R. (1996). Plyometric training in female athletes: Decreased impact forces and increased hamstring torques. American Journal of Sports Medicine, 24, 6, 765–773.
Kendall, F.P., et al. (2005). Muscles Testing and Function with Posture and Pain (5th ed.). Lippincott, Williams and Wilkins: Baltimore, Md.
Kreighbaum, E. and Barthels, K.M. (1996). Biomechanics: A Qualitative Approach for Studying Human Movement (4th ed.) A Pearson Education company: Needham, Mass.
Lohmander, L.S., Englund, P.M., Dahl, L.L. and Roos, E.M. (2007). The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. American Journal of Sports Medicine, 35, 10, 1756–1769.
Lal, S. and Hoch, A, (2007). Factors that affect the young female athlete. Physical Medicine and Rehabilitation Clinics of North America, 18, 361–383.
Lindenfeld, T.N., et al. (1994). Incidence of injury in indoor soccer. American Journal of Sports Medicine, 22, 8, 364–371.
McGill, S.M. (2006). Ultimate Back Fitness and Performance (3rd ed.). Wabuno Publishers: Waterloo, Ontario.
Myer, G.D., et al. (2008). The effects of generalized joint laxity on risk of anterior cruciate ligament injury in young female athletes. American Journal of Sports Medicine, 36, 6, 1073–1080.
Noyes, F.D., et al. (2005). The drop-jump screening test: Difference in lower limb control by gender and effect on neuromuscular training in female athletes. American Journal of Sports Medicine, 33, 2, 1197–1207.
Parkkari, J., et al. (2008). The risk for a cruciate ligament injury of the knee in adolescents and young adults: a population-based cohort study of 46 500 people with a 9-year follow-up. British Journal of Medicine, 42, 6, 422–426.
Renstrom, P., et al. (2008). Non-contact ACL injuries in female athletes: an International Olympic Committee current concepts statement. British Journal of Medicine, 42, 6, 394–412.
Sahrmann, S.A. (2002). Diagnosis and Treatment of Movement Impairment Syndromes. Mosby: St. Louis, Mo.
Schmidt, R.A. and Wrisberg, C.A. (2004). Motor Learning and Performance (3rd ed.). Human Kinetics: Champaign, Ill.
Walsh, J.C., et al. (2007).Three-dimensional motion analysis of the lumbar spine during “free squat” weight lift training. American Journal of Sports Medicine, 35, 927-932.
Whiting, W.C. and Rugg, S. (2006). Dynatomy – Dynamic Human Anatomy. Human Kinetics: Champagne, Ill.
Wilthrow, T.J., Huston, L.J., Wojtys, E.M. and Ashton-Miller, J.A. (2005). The relationship between quadriceps muscle force, knee flexion and anterior cruciate ligament strain in an in vitro simulated jump landing. American Journal of Sports Medicine, 34, 2, 269–274.