
BY FABIO COMANA, M.A., M.S.
This is the second article in a four-part series covering the new ACE Integrated Fitness Training Model.
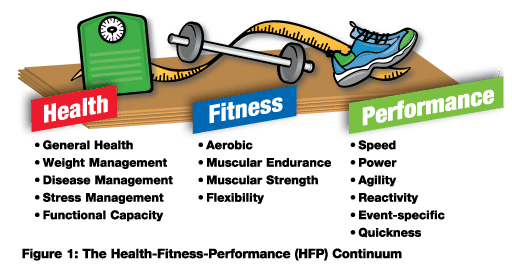
While all clients seek goals that vary along the health–fitness–performance continuum (Figure 1), they all fundamentally share one training objective: to improve their efficiency of movement.
Although forward progress through this continuum is logical, it is the responsibility of the fitness professional to assess the appropriateness of progression and consider the need for initial regression that addresses the foundational elements of restoring good posture, improving stability and mobility throughout the kinetic chain, reestablishing core function, developing balance and promoting movement efficiency.
The ACE Integrated Fitness Training (IFT) Model not only encompasses the current scope of practice for personal trainers, coaches and practitioners, but also includes a programming blueprint to address the need for stability and mobility, and for training movement. Additionally, the model addresses the notion of dysfunctional fitness, a concept gaining greater attention among fitness professionals. As technology continues to advance the complexity of exercise equipment, many exercises and drills have become equally technical, increasing the potential for poor technique, overuse and injury. As most deconditioned adults exhibit limited mobility and stability throughout the kinetic chain, they resort to compensated movement patterns when performing complex exercises or when using advanced equipment. This raises the concern whether exercise, without regard to the individual’s levels of stability and mobility or their movement efficiency, is actually doing more harm than good.
The first two phases of the ACE IFT Model serve as a critical foundation to all training and is the basis from which load and performance training should begin. The goal of this article is to discuss key concepts of each phase and introduce a template developed within the IFT model that progresses individuals in preparation for more traditional load and performance training. (See the February/March 2010 issue of ACE Certified News for an overview of the entire ACE IFT Model.) It should be noted that educating clients and athletes on the importance of this foundation can prove challenging. Fitness professionals can address this need by emphasizing both the short- and long-term benefits to fitness, performance and overall quality of life. While clients present with goals consistent with load training, they may require a few weeks to months of initial training emphasizing these prerequisites. This does not disqualify them from performing resistance training, but we must recognize this need and temporarily de-emphasize load or volume training with external resistance. Load or volume training without first addressing these prerequisites may exacerbate existing compensations and dysfunction.

Before discussing programming components of each phase, it may be useful to first define the terms.
- Joint stability is the ability to maintain or control joint movement or position. This is achieved by the synergistic actions of the components of the joint (e.g., muscles, ligaments, joint capsule) and the neuromuscular system, but must never compromise joint mobility.
- Joint mobility is the range of uninhibited movement around a joint or body segment. This is also achieved by the synergistic actions of the joint components and neuromuscular system, and also must never compromise joint stability.
Movement generally begins from a position of good, static posture. While all joints demonstrate varying levels of stability and mobility, they generally favor one over the other depending on their function. For example, the hips are highly mobile, demonstrating significant movement in all three planes, whereas the lumbar spine is more stable, demonstrating limited ranges of movement. Likewise, the glenohumeral joint is highly mobile, whereas the scapulo-thoracic region is more stable, providing a solid platform from which upper-extremity pulling and pushing movements occur. If we examine the relationship of stability and mobility throughout the kinetic chain, we note an interesting relationship exists (Figure 2).
Individuals who exhibit good posture with muscle balance generally demonstrate an appropriate relationship between stability and mobility throughout the kinetic chain. Concerns arise, however, with individuals who exhibit poor posture and muscle imbalances. What happens to joint movement along the kinetic chain when appropriate levels of mobility are lacking?
Adjacent, more stable joints may need to compromise some degree of stability to facilitate the level of mobility needed at the moving joint. For example, if a client exhibits excessive kyphosis (loss of thoracic mobility) and attempts to extend the thoracic spine, the body may resort to increasing lumbar lordosis to compensate for the lack of thoracic mobility.
A moving joint will seek to achieve the desired range of motion by incorporating movement into other planes. For example, if a client performs a hip-extension movement (sagittal plane) and lacks flexibility within the hip flexors, external rotation of the leg and hips into the transverse plane may occur, producing a compensated movement pattern.
Phase 1: Stability and Mobility
The primary objective of Phase 1 is to reestablish appropriate levels of stability and mobility within the kinetic chain, beginning with the most proximal region of the body and gradually progressing toward the distal segments. Figure 3 presents a template for this progression.
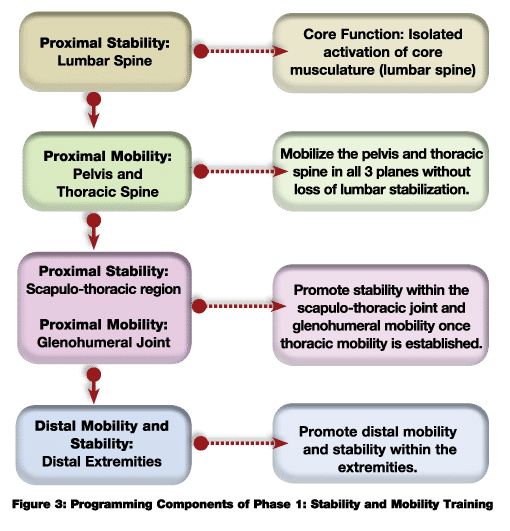
The lumbar spine is most proximal to the body’s center of mass (COM) and the core. Programming should focus initially on promoting stability of the lumbar region through the actions and functions of the core. Given the impact of poor posture upon muscle hypertonicity (tight lumbar extensors), there may also be a need to promote muscle extensibility by stretching the lumbar extensors (e.g., using cat-camels). Once some stability in this region is achieved, the focus of the program should shift to addressing adjacent segments; specifically the hips and thoracic spine; then stability within the parascapular muscles of the scapula-thoracic region; and, finally, mobility throughout the distal segments. Attempting to improve a client’s mobility within distal joints without first developing proximal stability will likely compromise stability within these segments. Without appropriate joint stability, muscles normally involved in mobilization of a joint may need to alter function and offer stability to the joint. For example, a lack of scapula-thoracic stability may force the deltoids, normally responsible for glenohumeral movement, to compromise their force-generating capacity and assist with scapular stability. For more in-depth information on this subject, refer to Chapter 9 of the ACE Personal Trainer Manual (4th edition).
Programming Guidelines for Phase 1
Consider the following basic guidelines when programming within Phase 1:
1. Promote conscious awareness of postural deviations.
- Posture is controlled subconsciously by lower portions of the brain, and most individuals who exhibit poor posture are not consciously aware of their alignment.
- Conscious awareness shifts control to higher regions of the brain and helps reeducate faulty neural information. This is a critical first step to restoring good posture.
2. Distinguish between correctible and non-correctible postural compensations.
- Most compensations and muscle imbalance originate from correctible factors, including inactivity, repetitive motions, awkward positions, work environment, side dominance, improper exercise technique and poorly designed training programs. However, some can be attributed to non-correctible or potentially non-correctible factors, such as congenital conditions (e.g., scoliosis), pathologies (e.g., rheumatoid arthritis), structural deviations (e.g., tibial torsion, femoral anteversion), or trauma (e.g., surgery, injury, amputations).
- Coach; don’t manually move the joint, but rather ask the client to move his or her joint according to your cues.
3. Evaluate the client’s intention to make lasting improvements.
- Working with your client for three hours a week to improve posture can be negated quickly if he or she does not make any real commitment to change during non-training hours.
4. Always respect scope of practice and the need for referral to qualified professionals.
- You are not qualified to diagnose injuries or medical conditions. If your client is experiencing musculoskeletal pain, refer him or her for medical evaluation.
5. The time required to successfully establish stability and mobility depends upon individual differences such as current conditioning level, past experiences, body type, abilities, attitudes, adherence, motivational levels, emotional make-up, learning style and maturation level.
6. A deconditioned individual generally lacks the ability to stabilize his or her own body.
- The initial emphasis in restoring good posture and this relationship of stability and mobility should focus upon muscle isolation in a supported environment (e.g., using the floor, walls, back rests) before introducing integrated (whole-body, unsupported) exercises.
- The use of supports also offers an additional benefit of kinesthetic and visual feedback critical to helping clients understand alignment of specific joints (e.g., when lying on the floor the individual can feel the contact points with the floor when joints are placed in a good postural position).
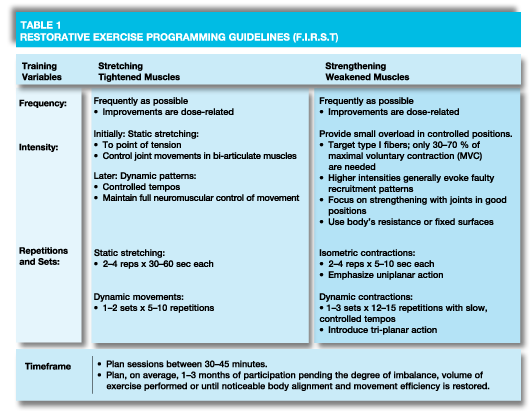
7. Restoring good posture essentially involves improving extensibility in the tightened, hypertonic muscles, while improving muscular endurance (targeting type 1 fibers) in the weakened postural (tonic) muscles. However, it is not as simple as just stretching tight muscles and strengthening weak muscles. Physiological and morphological changes will establish kinetic chain stability and mobility. These concepts are discussed in detail in the ACE Personal Trainer Manual (4th edition).
- The tightened muscles need to undergo a morphological change to add sarcomeres back in series within the myofibrils, which re-establishes the muscle’s normal length-tension relationship.
- Following current ACSM guidelines for flexibility is generally insufficient to bring about these changes.
- Passive elongation for sustained time periods (as long as possible), coupled with conscious awareness of proper joint alignment, are keys to success.
- This will reduce nerve tonicity (nerve tone) of the muscle and establish normal neural function (neural re-education).
- Weakened (lengthened muscles) must also undergo a morphological change to reestablish the muscle’s normal length-tension relationship and promote a healthy force-coupling relationship at the joint.
- Traditional strength training involving dynamic movements and full ranges of motion are not optimal for facilitating the initial adaptations needed for good posture.
- Target type 1 fibers within the postural muscles by implementing sustained-duration isometrics or lower-intensity, higher-volume dynamic contractions.
- Isometrics are favored as the muscle is strong in the lengthened position, but weak where it needs to maintain good posture. By contrast, dynamic movement may utilize momentum to power muscles through weaker positions (Table 1).
Phase Two: Movement
Engrams are presumed encodings that occur within neural tissue that provide a physical basis for the persistence of memory. Learned movement patterns are essentially stored engrams that we call upon to perform our activities of daily living, yet we possess the capability to fine tune them as needed to meet the demands of the task performed. Consequently, the notion of training and coaching movement patterns rather than teaching exercises appears to provide a solid foundation to training. Human movement can essentially be broken down into five primary movements that encompass all activities of daily living (ADL):
- Single-leg movements (e.g., single-leg stance and lunging)
- Bend-and-lift movements (e.g., squatting)
- Pushing movements (primarily in the
vertical/horizontal planes)
- Pulling movements (primarily in the
vertical/horizontal planes)
- Rotational (spiral) movements
Movements can be as simple as a single primary movement or as complex as combining several into an integrated movement pattern. Consider, for example, a woman picking up her child and then turning to place the child in a highchair. She performs a bend-and-lift movement; a rotational movement; a single-leg movement to walk; a pushing movement extending her arms to place her child in the highchair; and a pulling movement to resist gravity while lowering her child into the highchair.
As we spend the majority of our day moving our own body, bodyweight training is the most appropriate modality to use during this stage. However, it is appropriate to include some light resistance to increase system overload once the client develops good form in performing the primary movement patterns. Segment learning of each movement pattern utilizing the part-to-whole approach and introduce progressions appropriately:
- While most ADL are performed with the lower extremity operating in a closed-chain environment (e.g., moving against the floor) and the upper-extremity operating in an open-chain environment (e.g., pushing and pulling on doors), the initial use of supports offers greater kinesthetic awareness to movement quality. Coupled with visual feedback, this helps cue the clients to improving their movement efficiency.
- Incorporate extremities and the head/torso as drivers to increase system overload, balance, and additional stability and mobility demands (e.g., driving both arms towards the floor during a bend-and-lift movement).
- Teach movement in all three planes, beginning with the sagittal plane, then the frontal plane and lastly the transverse plane.
- Introduce three-dimensional demands upon the body, both in the stable, closed-chain and freely moving, open-chain segments (e.g., performing a bend-and-lift movement in a staggered-stance position with the lead leg positioned in slight internal rotation while driving the upper extremity in the transverse plane).

During this phase, it is critical to coach movement effectively. We must always understand the objective behind every movement pattern or exercise we program, as well as the role of individual body segments within the kinetic chain required to perform that movement or pattern. The acronym M.O.V.E. can be used to teach movement patterns effectively (Figure 4).
For example, when performing a bird-dog movement, you should first identify what joint movements and planes of movements are desired (e.g., Which joints should remain stable and which are mobile? Is the movement in the sagittal or frontal plane?)
Once you have explained and demonstrated the movement, allow the client to practice and observe his or her performance. You must identify whether the desired movements occurred (e.g., Did the lumbar spine remain stable during hip extension? Was there rotation through the hips?). Next, and most importantly, you must validate why the compensations occurred (e.g., Was the increased lordosis during hip extension due to a lack of core stabilization, or a lack of hip flexibility, or both?). Finally, your ultimate responsibility is to educate the client to correct his or her form by identifying problematic areas and segment learning as needed.
As with Phase 1, the timeframe needed to train these movements successfully depends on individual differences, including current conditioning level, past experiences, body type, abilities, attitudes, motivational levels, emotional make-up, learning style and maturation level.
Once your client demonstrates movement efficiency, he or she is ready to move into Phase 3—the Load Training phase—of the ACE IFT Model. However, many of the three-dimensional movement patterns with various progressions should remain part of the client’s maintenance plan to continually reinforce good movement habits. Incorporate these movements into dynamic warm-ups, structure them as complementary drills (exercises) to the client’s Phase 3 or 4 workouts or even program them as complete stand-alone sessions.
Phases 3 and 4 of the ACE IFT Model will be discussed in part three of this series.
_____________________________________________________________

Fabio Comana, M.A., M.S., is an exercise physiologist and spokesperson for the American Council on Exercise, and faculty at San Diego State University (SDSU) and the University of California San Diego (UCSD), teaching courses in exercise science and nutrition. He holds two master’s degrees, one in exercise physiology and one in nutrition, as well as certifications through ACE, ACSM, NSCA, and ISSN.