BY TODD GALATI, M.A.
This is the first article in a four-part series covering the new ACE Integrated Fitness Training Model.

What if . . .
. . . personal training could consistently provide positive and memorable experiences that would drive participation and retention?
. . . personal trainers could align their communication styles to each client’s personality index to promote trust and facilitate effective dialogue?
. . . personal trainers could gain a better understanding of, and uniquely program for, each client’s cognitive, emotional and physiological characteristics?
. . . personal trainers could effectively determine readiness to change behavior and then implement effective strategies to promote healthy behaviors and program adherence?
. . . there was a simple, yet systematic approach to programming that was relevant, appropriate, effective, and adaptable for any client?
. . . there was a logical and customized progression for all individuals for cardiorespiratory, functional movement, resistance, balance, flexibility and core training?
These “what if” statements represent some of the key challenges ACE hears regularly from personal trainers, managers, directors, club owners and educators. Solutions are needed for each of these questions if the fitness industry is going to move ahead from the practices of yesterday into the next decade and beyond.
After years of reviewing industry research, consulting with numerous subject-matter experts in the fitness industry, and then trying to design solutions for each of these questions, the exercise scientists at the American Council on Exercise posed the following challenge to themselves: What if there was one blueprint for all of this?
To address such a large challenge, ACE adopted a “blue-sky” approach to planning by first formulating a vision of what a comprehensive plan for successful personal training would look like. This comprehensive blueprint would need to be applicable for novice and veteran personal trainers, personal-training managers and directors, club owners and educators, and it would need to apply to clients across the full spectrum of the health–fitness–performance continuum. Additionally, this blueprint would need to incorporate scientifically proven practices, while eliminating antiquated methods that create barriers to client enjoyment of, and adherence to, exercise.
The Evolution of Personal Training
Personal training has gone through a significant evolution during the past 25 years, transforming from a relatively straightforward profession into a multifaceted field in allied healthcare. Today, personal trainers must meet the mounting challenges of an aging and increasingly overweight population with a long list of special needs that includes cardiovascular disease, hypertension, diabetes, metabolic syndrome and a variety of orthopedic conditions, including osteoporosis, osteoarthritis, low-back issues and post-orthopedic rehabilitation.
Advances in exercise science and medical research have led to updated exercise guidelines for both apparently healthy and special needs clientele. These guidelines provide broad parameters for programming, but lack the specific details necessary for unique programming based on each client’s goals and current level of health and fitness. They also fail to address the diverse motivational needs of special population clientele who may have a history of exercise successes and failures or may be dealing with limited functional capacities.
Today, effective personal trainers must first build rapport with their clients, and then match the appropriate motivation and communication techniques with the right exercise program to help clients adopt healthful behaviors, build self-efficacy and safely reach their goals. This has evolved personal training from a science to an art form that incorporates the science of exercise with strong communication and teaching techniques that complement the psychological, emotional and physiological needs and concerns of their clients. This transition has new professionals, seasoned veterans, educators, and club owners and managers wondering how to pull it all together for themselves and their clients, employees and students.
ACE Integrated Fitness TrainingTM Model
The American Council on Exercise developed the ACE Integrated Fitness TrainingTM (ACE IFTTM) Model to provide personal trainers with a systematic and comprehensive approach to exercise programming that integrates assessments and programming to facilitate rapport, adherence and behavior change, while also improving posture, movement, flexibility, balance, core function, cardiorespiratory fitness, muscular endurance and muscular strength.
The ACE IFT Model organizes the latest exercise science research into a logical system that helps trainers determine appropriate assessments, exercises and progressions for clients based on their unique health, fitness, needs, goals and readiness to change behavior. The ACE IFT Model has two principal training components:
- Functional movement and resistance training
- Cardiorespiratory training
Each component is comprised of four phases (Figure 1) that provide trainers with a system for determining and implementing the most appropriate assessments, exercise programs, progressions and regressions for clients at all fitness levels. Rapport is the foundation for success during every phase, whether a trainer is working with a competitive athlete or a previously sedentary client just beginning an exercise program.
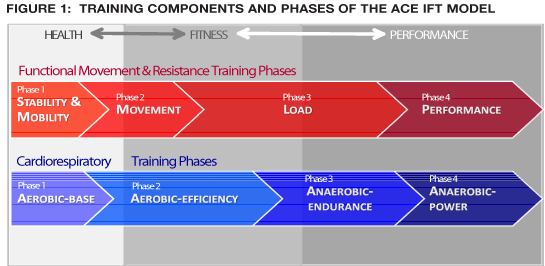
The four training phases span the full health–fitness–performance training continuum, which is based upon the premise that exercise programs should follow a logical progression that first improves health, then develops and advances fitness, and finally enhances performance. Each client will be at a unique point on the continuum and should be progressed according to his or her available time, capacity for recovery and outside stressors such as work, family and travel. Clients who have been sedentary for years should initially focus on becoming regular exercisers to improve health before progressing to work on improving fitness. This should seem logical, but what about the avid weight lifter or long-time runner? Should a client fitting one of these profiles automatically train all exercise parameters at intensities that fall into the fitness or performance domains? The ACE IFT Model provides the answers to these types of questions for clients at all points along the health–fitness–performance continuum.
Rapport
The greatest impact a personal trainer can have on a client’s life is to help that person adopt new fitness-related behaviors and establish a positive relationship with exercise. For this reason, rapport is the foundation of the ACE IFT Model. By developing this critical component of the client–trainer relationship, personal trainers can promote open communication, develop trust and foster the client’s desire to participate in an exercise program. Rapport should be developed early through open communication and initial positive experiences with exercise, and then enhanced through behavioral strategies that facilitate long-term adherence.
Exercise programming has traditionally focused on physiological changes, placing early emphasis on fitness assessments for program design and tracking progress. Some assessments are critical for ensuring client safety and designing appropriate exercise programs, but do personal trainers really need to conduct a full battery of physiological assessments with each client? The answer is no. While it is true that programming has traditionally depended on baseline values to assess progress, this practice can be counterproductive to client motivation and adherence.
Conducting a comprehensive set of physiological assessments can be detrimental to early program success by reinforcing a client’s negative self-image and beliefs that he or she is out of shape or overweight. Do obese clients who want to lose significant weight really need to have their skinfolds measured to confirm what they already know? Does a client who cannot walk for more than 10 continuous minutes really need to perform a test of cardiorespiratory fitness? If the client is high risk, he or she should be referred for a medical examination and a graded exercise test prior to participating in an exercise program. But if the client is at moderate risk and just has poor fitness, walking for up to 10 continuous minutes is both a fitness assessment and a workout. This does not negate the effectiveness of fitness assessments. They are good tools for assessing progress, but personal trainers must always determine which fitness assessments to use with each client based on his or her current fitness, goals and desire for assessment.
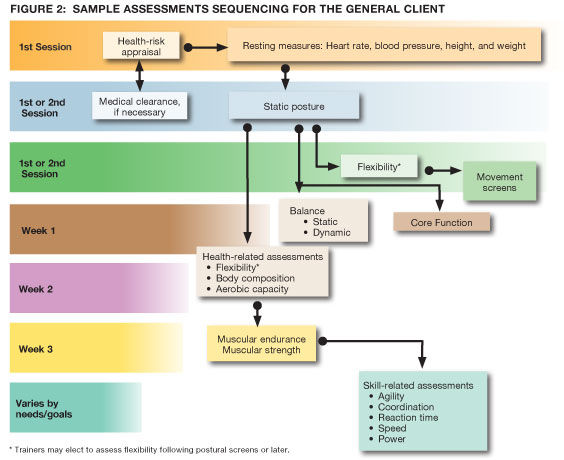
Personal trainers should always collect health-history information to determine if the client has any contraindications or requires a physician’s evaluation prior to exercise. The ACE IFT Model includes functional and physiological assessments that can be performed during specific phases to provide information for exercise programming in that phase. Some assessments, such as those that focus on functional movement, balance and range of motion, may be conducted within the first few sessions with a new client, while other assessments should wait until the client has progressed from one phase to another. Ideally, trainers should utilize a sequential approach to conducting assessments that begins with reviewing the client’s health history, discussing desires, preferences and goals, completing a needs assessment, and then determining relevant assessments and timelines for conducting them (Figure 2).
At the first client–trainer meeting, it is important to encourage the client and create an environment where he or she can feel successful. It is also important for the trainer to be mindful that many adults have been inactive since childhood. After two to four weeks of regular physical activity, clients will generally experience more stable positive moods due to:
- Changes in hormone and neurotransmitter levels (e.g., endorphins, serotonin, norepinephrine)
- Increased self-efficacy with task and possibly short-term goal accomplishment
- Improved performance due to neuromuscular adaptations to exercise
These positive factors will enhance adherence behaviors, but the client must make it through two to four weeks of regular exercise to reap these benefits. To help a client transition to the action stage of behavior change, the trainer should make exercise fun and emphasize regular adherence first before switching the primary focus toward any other goals such as weight loss or body-composition changes. By providing regular positive experiences with exercise, personal trainers can help clients to have continued success.
Functional Movement and Resistance Training
Functional movement and resistance training are often treated as two separate types of training, even though resistance training is the application of an external load to movements. In the ACE IFT Model, they form one training component that progresses from training to improve postural stability and mobility to performance training (Table 1). Individuals who have weak core muscles or postural imbalances are at increased risk for injury when applying external loads to their movements. For that reason, phase 1 of this training component is focused on assessments and training for postural and joint stability and mobility. Once clients gain good postural integrity, they can progress to phase 2, where assessments and training are focused on good movement patterns. Once clients can perform proper movement sequences, they can progress to phase 3, where external loads are applied to movements. Only clients who have progressed to advanced training in phase 3 and have performance-oriented goals will move on to phase 4.
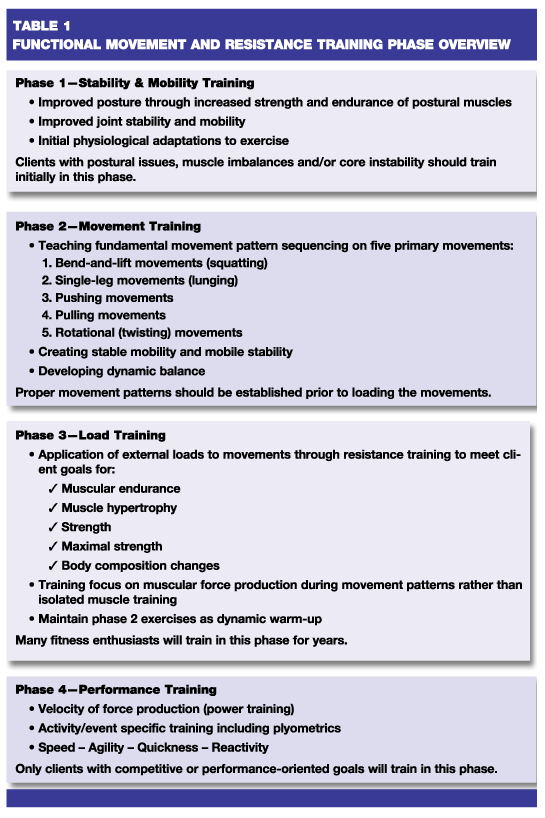
Many clients, regardless of their current exercise frequency and fitness level, will have muscle imbalances, postural issues and improper movement mechanics that should be addressed through early stability and mobility training and then progress to movement training. This will require some clients to regress from load training back to phase 1 training. The personal trainer can facilitate this by communicating the benefits of improved core function, postural and joint stability and mobility, and movement patterns on health, as well as performance once the client resumes load training.
Cardiorespiratory Training
Cardiorespiratory-training programs have traditionally focused on steady-state training to improve cardiorespiratory fitness, with workload generally progressed through increased duration and/or intensity, and the use of loosely categorized intervals with a primary focus on reducing boredom, or training intervals at or near the lactate threshold to improve speed during endurance events. The ACE IFT Model provides a systematic approach to cardiorespiratory training that can take a client from being sedentary to training for a personal record in an event such as a half-marathon. While this will not be the goal of most clients, having an organized system that can allow for long-term progression like this is empowering for the personal trainer (Table 2).
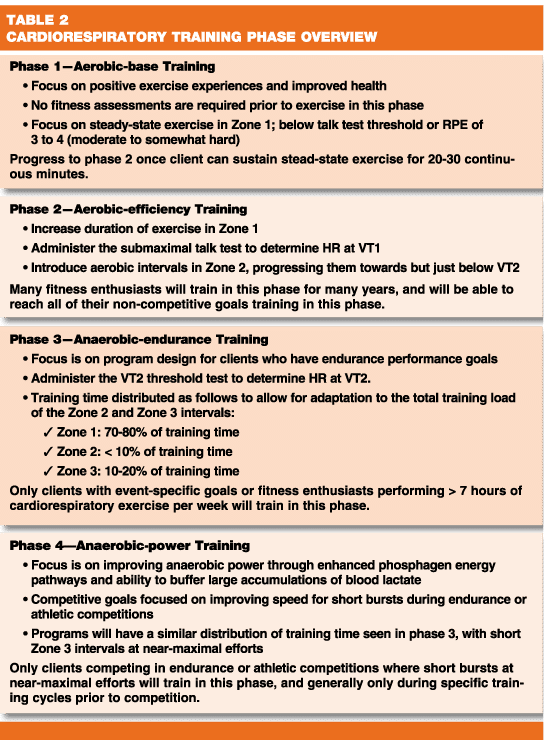
This training component begins with the development of an initial aerobic base to improve health and then progresses to improving cardiorespiratory fitness through aerobic-efficiency training in phase 2, which is where many clients will train for years. Clients with competitive endurance goals will progress to anaerobic-endurance training in phase 3, and only those clients with specific needs for near-maximal speed during endurance events or competitive start-stop sports activities will train for anaerobic-power in phase 4.
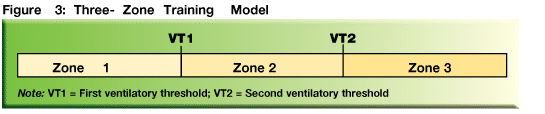
Cardiorespiratory training in the ACE IFT Model uses client-specific intensity markers that include the talk test, heart rate at the first and second ventilator thresholds (VT1 and VT2), and ratings of perceived exertion. Traditional intensity markers such as percentages of maximal heart rate (%MHR), heart rate reserve (%HRR), or V•O2 reserve (%V•O2R) are not recommended for use with the ACE IFT Model because of the inherent error of predicted MHR and predicted V•O2max. Instead, training parameters are set around a three-zone model (Figure 3):
Zone 1: HR < VT1.
Zone 2: HR = VT1 to HR < VT2.
Zone 3: HR > VT2.
During each cardiorespiratory training phase the modes of exercise performed should accommodate the level of exertion required, while also being appropriate for the client’s preferences, health, fitness and contraindications.
ACE IFT Model for Special Population Clientele
Personal trainers in most settings will work with clients who have a variety of special needs. Once these clients have been cleared for exercise by their physicians, trainers can utilize the integrated training process of the ACE IFT Model by adjusting exercise selection, intensity, sets, repetitions and duration to fit the needs of each client based on his or her physician’s recommendations and the guidelines available for his or her specific condition. Depending upon the condition, a special-needs client may progress normally or may stay in a training phase for a long time. The most important goal is to provide each client with initial positive experiences that promote adherence through easily achieved initial successes. Transitioning a special-population client into first the action and then the maintenance stages of change will have a significant impact on that client’s health and quality of life.
Summary
The ACE Integrated Fitness Training Model provides a systematic approach for utilizing distinct training mesocycles (phases) and progressions with unique points of entry for all clientele. The ACE IFT Model also includes key behavioral and emotional strategies to enhance the overall exercise experience. This comprehensive system is ideal for novice trainers, yet accommodates practices of experienced trainers, managers and directors, and it provides a logical approach for educators teaching students the application of program design and progression. And, the ACE IFT Model can be used to enhance the business of personal training through a closed-end sales and marketing approach to selling personal training packages and promoting staff expertise in the various training phases.
Interested in learning more about the ACE IFT Model? Take the free ACE IFT online course and earn 0.1 CECs.
References
American College of Sports Medicine (2010). ACSM’s Guidelines for Exercise Testing and Prescription (8th ed.). Philadelphia: Lippincott Williams & Wilkins.
American Council on Exercise (2009). ACE Advanced Health & Fitness Specialist Manual. San Diego, California: American Council on Exercise.
American Council on Exercise (2008). ACE Lifestyle & Weight Management Consultant Manual. San Diego, California: American Council on Exercise.
Esteve-Lanao, J. et al. (2007). Impact of training intensity distribution on performance in endurance athletes. Journal of Strength and Conditioning Research, 21, 943–949.
Foster, C. (1998). Monitoring training in athletes with reference to overtraining syndrome. Medicine & Science in Sports & Exercise, 30, 1164–1168.
U.S. Department of Health and Human Services (2008). 2008 Physical Activity Guidelines for Americans: Be Active, Healthy and Happy. www.health.gov/paguidelines/pdf/paguide.
_______________________________________________________________________

TODD GALATI, M.A., is the certification and exam development manager for the American Council on Exercise and serves on volunteer committees with the Institute for Credentialing Excellence, formerly the National Organization for Competency Assurance. He holds a bachelor’s degree in athletic training and a master’s degree in kinesiology and four ACE certifications (Personal Trainer, Advanced Health & Fitness Specialist, Lifestyle & Weight Management Consultant, and Group Fitness Instructor).