
By Lance C. Dalleck, Ph.D.
Cardiovascular diseases (CVD), such as coronary artery disease, account for more than 17 million deaths worldwide each year, representing nearly one-third of the annual death toll. The risk of mortality from heart disease can be significantly reduced by positively modifying various CVD risk factors that contribute to the progression of the disease. Historically, prevention and rehabilitation exercise programs have been designed with the intent to lower blood pressure and reduce excess levels of cholesterol and fat mass. While hypertension, high cholesterol and obesity undoubtedly contribute to heart-disease risk, more recent research suggests that there may be an even more powerful predictor of heart disease: cardiorespiratory fitness. It has recently been shown that low levels of cardiorespiratory fitness better predicts an individual’s risk of developing heart disease and heart-disease mortality compared to traditional CVD risk factors. This article examines the growing body of research highlighting low cardiorespiratory fitness as a critical CVD risk factor, and presents key training requirements for optimizing this ultimate health outcome.
Cardiorespiratory Fitness: A Risk Factor for CVD?
Cardiorespiratory fitness, typically determined by measuring maximal oxygen uptake, or VO2max, refers to the highest rate at which oxygen can be taken up and consumed by the body during intense exercise. Historically, the magnitude of an individual’s VO2max has been viewed as one of the most important predictors of endurance exercise performance. A classic study conducted in the 1970s at Ball State University confirmed the importance of VO2max to endurance exercise performance, with findings indicating a strong correlation between VO2max and 10-mile run times (Costill, 1970). Although it seems logical to assume that an individual with high levels of cardiorespiratory fitness will also have good cardiovascular health, it is interesting that low cardiorespiratory fitness is not usually recognized as a CVD risk factor. For instance, the American College of Sports Medicine (ACSM, 2010) uses eight factors to stratify individuals into low-, moderate- or high-risk categories: age, smoking, obesity, impaired fasting blood glucose, dyslipidemia, family history, sedentary lifestyle and hypertension. Cardiorespiratory fitness is notably absent from this risk-stratification schema, as it is from many other CVD risk-factor lists. However, a wealth of research findings accumulated over the past quarter century may soon change things. In fact, cardiorespiratory fitness recently was coined the ultimate marker for risk stratification and health outcomes (Franklin, 2007).
The Evidence
One of the very first studies to explore the connection between cardiorespiratory fitness and heart health was published in 1989. This hallmark paper reported that an inverse relationship existed between VO2max values and risk for CVD (Blair et al., 1989); similar findings were reported by Blair et al. in 1996. In both studies, these relationships held true for individuals with no other risk factors for CVD, one risk factor for CVD, and two or more CVD risk factors. More recently, the question of whether cardiorespiratory fitness should be considered a separate risk factor, in addition to lack of physical activity, was addressed in a meta-analysis (a statistical method that combines the results of numerous studies). The author noted that both increased cardiorespiratory fitness and increased physical activity were associated with decreased risk for CVD events (Williams, 2001). Interestingly, it was also found that higher cardiorespiratory fitness levels yielded greater reductions in CVD risk compared to those imparted from increased physical-activity levels. Therefore, it was concluded that being unfit warrants consideration as a separate CVD risk factor—independent of physical inactivity and other traditional CVD risk factors—and merits screening and intervention.
In 2005, researchers reported findings from a study that examined the effect of cardiorespiratory fitness on risk of mortality from CVD in a cohort of diabetic men within normal weight, overweight and obese categories (Church et al., 2005). Both diabetes and obesity are associated with increased risk of mortality from CVD. For all weight categories (normal, overweight and obese) it was shown that the risk of CVD mortality was two- to four-times higher among diabetic men with low levels of cardiorespiratory fitness compared to those with moderate-to-high levels of cardiorespiratory fitness.

Perhaps the strongest case to support cardiorespiratory fitness as the ultimate health outcome was made in a paper published in 2009. The author presented data to show that low cardiorespiratory fitness accounted for more overall deaths, including those from CVD, when compared to deaths that could be attributed to traditional risk factors, such as obesity, smoking, hypertension, high cholesterol and diabetes (Blair, 2009). Clearly, sufficient levels of cardiorespiratory fitness should be considered paramount to overall health. But at what point should you become alarmed with the cardiorespiratory fitness level of your clients?
Low Cardiorespiratory Fitness: How Low Is Too Low?
In addition to training status, the magnitude of an individual’s cardiorespiratory fitness level is dependent on numerous variables, including age, sex, race and genetics. Table 1 includes normative values for VO2max with specific reference to age and sex. In the previous section it was shown that low cardiorespiratory fitness is a powerful risk factor for CVD. But how low is too low? Williams (2001) noted that the highest relative risk of CVD existed for those individuals with cardiorespiratory fitness levels below the 20th percentile. Perhaps equally important is the fact that the most substantial drop in CVD risk involves just moving your client from the 20th to the 30th percentile. Put more simply, it is not necessary to turn your clients into Lance Armstrong to make them heart healthy! The case study featured in the sidebar below puts these findings into more functional terms, while the subsequent section examines why increased cardiorespiratory fitness levels lowers one’s risk for CVD.
Table 1. Normative Values for Maximal Oxygen Uptake (mL/kg/min)
|
| |
Age |
| Percentile* |
20–29 |
30–39 |
40–49 |
50–59 |
60–69 |
| Men |
|
|
|
|
|
|
90
|
54.0 |
52.5 |
51.1 |
46.8 |
43.2 |
| 80 |
51.1 |
48.9 |
46.8 |
43.3 |
39.5 |
| 70 |
48.2 |
46.8 |
44.2 |
41.0 |
36.7 |
| 60 |
45.7 |
44.4 |
42.4 |
38.3 |
35.0 |
| 50 |
43.9 |
42.4 |
40.4 |
36.7 |
33.1 |
| 40 |
42.2 |
41.0 |
38.4 |
35.2 |
31.4 |
| 30 |
40.3 |
38.5 |
36.7 |
33.2 |
29.4 |
| 20 |
39.5 |
36.7 |
34.6 |
31.1 |
27.4 |
| 10 |
35.2 |
33.8 |
31.8 |
28.4 |
24.1 |
| Women |
|
|
|
|
|
|
90
|
47.5 |
44.7 |
42.4 |
38.1 |
34.6 |
| 80 |
44.0 |
41.0 |
38.9 |
35.2 |
32.3 |
| 70 |
41.1 |
38.8 |
36.7 |
32.9 |
30.2 |
| 60 |
39.5 |
36.7 |
35.1 |
31.4 |
29.1 |
| 50 |
37.4 |
35.2 |
33.3 |
30.2 |
27.5 |
| 40 |
35.5 |
33.8 |
31.6 |
28.7 |
26.6 |
| 30 |
33.8 |
32.3 |
29.7 |
27.3 |
24.9 |
| 20 |
31.6 |
29.9 |
28.0 |
25.5 |
23.7 |
| 10 |
29.4 |
27.4 |
25.6 |
23.7 |
21.7 |
*To realize the health benefits of aerobic conditioning, personal-training clients should aim to achieve >30th percentile.
Note: VO2max below the 20th percentile is associated with an increased risk of death from all causes (Blair et al., 1995). Study population for the data set was predominately white and college-educated. A modified Balke treadmill test was used with VO2max estimated from the last grade/speed achieved. The following may be used as descriptors for the percentile rankings: well above average (90), above average (70), average (50), below average (30), and well below average (10). Reprinted with permission from The Cooper Institute, Dallas, Texas from Physical Fitness Assessments and Norms for Adults and Law Enforcement. Available online at www.cooperinstitute.org.
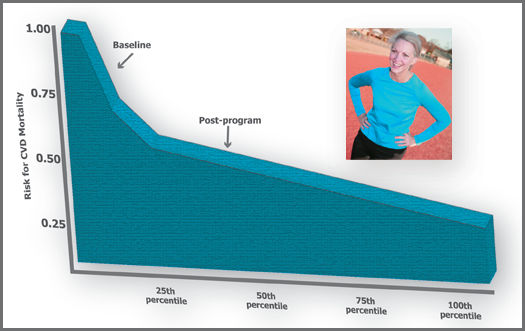
Case StudyAspen, a 49-year-old woman, begins an exercise program with a VO
2max value of 26.7 mL/kg/min, placing her in the 15th percentile according to her age and sex. This cardiorespiratory level places her in the highest category of risk because she is below the 20th percentile (Williams, 2001). After three months of training, her VO
2max increases by 15 percent to 30.9 mL/kg/min, which now places her in the 35th percentile based on her age and sex. Most importantly, this realistic improvement in her cardiorespiratory fitness level has reduced her risk for CVD mortality by 30 percent.
|
Baseline
|
Post-program
|
| VO2max |
26.7 |
30.9 |
| Percentile Rank |
15th |
35th |
| Risk Reduction |
— |
30% |
Why Do Higher Levels of Cardiorespiratory Fitness Equate to Reduced Risk of CVD?
A good VO2max does not simply mean we have the potential to complete a local road race—it also is indicative of heart health. But why? There are several reasons why the training adaptations that culminate with improved cardiorespiratory fitness concurrently augments skeletal muscle structure and function, which in turn contributes to reduced risk of CVD.
Increased Capillary Density
Increased cardiorespiratory fitness is associated with increased capillary density, which results in an enhanced ability to deliver oxygenated blood to exercising skeletal muscle (Gill and Malkova, 2006). It also means there is an increased capacity to deliver blood glucose to skeletal muscle where it can subsequently be taken up and used for energy or stored as glycogen. The capacity to dispose of blood glucose more effectively reduces the risk of impaired fasting blood glucose values and type 2 diabetes—both risk factors for CVD (ACSM, 2010).
Complete Breakdown of Fats
Insulin resistance is a metabolic abnormality in which the binding of insulin to receptors on the skeletal muscle membrane are blocked. This disrupts the transport of blood glucose into the muscle. As described earlier, this can lead to impaired blood glucose, and eventually type 2 diabetes. A main contributing factor to insulin resistance is the incomplete breakdown of fats that have entered into skeletal muscle cells (Horowitz, 2007). When this occurs, the body responds by turning on an inflammatory pathway that inhibits insulin binding. Some of the featured training adaptations that result in improvements to cardiorespiratory fitness include increased mitochondrial mass and number, as well as an increase in the various enzymes involved in mitochondrial respiration. These physiological changes in the skeletal muscle not only improve cardiorespiratory fitness, but also favor an increased capacity for fat metabolism. Accordingly, there is a decreased likelihood of an incomplete breakdown of fats entering into skeletal muscle, which subsequently reduces the activity of the inflammatory pathway contributing to insulin resistance (Horowitz, 2007).

Exercise Programming Considerations for Improving Cardiorespiratory Fitness
When formulating an exercise program specifically focused on improving cardiorespiratory fitness, consider the following three issues:
1. A minimal training intensity is required for a training adaptation to occur in terms of cardiorespiratory fitness.
2. There is a dose-response relationship between exercise volume and improvements in cardiorespiratory fitness.
3. High-intensity interval training (HIIT) can yield rapid improvements in cardiorespiratory fitness.
A Minimal Training Intensity
Regular physical activity confers numerous health benefits; however, for favorable training adaptations to occur, a minimal threshold intensity must be exceeded. The American College of Sports Medicine (ACSM, 2010) recommends an exercise intensity of 40−85% heart-rate reserve (HRR, which represents the difference between maximal heart rate and resting heart rate) or oxygen uptake reserve (VO2R, which represents the difference between maximal oxygen uptake and resting oxygen uptake). Importantly, unless the exercise intensity exceeds the lower end of this recommended range, meaningful improvements in cardiorespiratory fitness levels are unlikely to occur. It also is important to note that for less-fit individuals (those starting an exercise program with a cardiorespiratory fitness level below 40 mL/kg/min), research has shown these individuals will only need to exceed 30% of HRR or VO2R to experience a beneficial training effect (Swain and Franklin, 2002).
 A Dose-response Relationship
A Dose-response Relationship
Provided that the exercise intensity is sufficient, a favorable dose-response relationship exists between overall training volume and improvements in cardiorespiratory fitness (Garber et al., 2011). Simply put, the more time an individual allocates to aerobic-exercise training per week, the greater results one can expect. Two important questions to ask in terms of training volume are:
1. What is the minimal amount?
2. What is the optimal amount required for positive training adaptations?
Research has shown that moderate-intensity (40−50% HRR or VO2R) exercise sessions of 15 minutes per day, performed five days per week, result in significant improvements in cardiorespiratory fitness (Church et al., 2007). This weekly training volume of 75 minutes per week is likely approaching the minimal amount of aerobic exercise necessary to induce a training benefit. Determining an optimal amount of training volume is a more difficult proposition and one research has yet to fully elucidate. Nevertheless, it has been shown that in a dose-response manner, as weekly training volume increases from 30 minutes per day to 45 minutes per day, on five days per week at moderate intensity, cardiorespiratory fitness continues to improve.
Although it is probable that increased training volume for 60 minutes per day on most days of the week will yield even greater increases in cardiorespiratory fitness, this has yet to be studied in a carefully controlled manner.

High-intensity Interval Training
One of the classic methods for eliciting improvements in cardiorespiratory fitness is through high-intensity interval training (HIIT). This tactic has long been a staple of training programs for endurance athletes; however, only recently has this practice found its way into the workout regimen of everyday fitness enthusiasts. Recent research has demonstrated that quick and impressive improvements in cardiorespiratory fitness can be amassed with HIIT. For example, one study reported a 20 percent improvement in cardiorespiratory fitness in only six weeks of HIIT (Gormley et al., 2008). Nonetheless, you should practice a degree of caution when considering adding HIIT to your clients’ exercise programs. Although no adverse effects of HIIT have been reported in the literature, the long-term effects and safety of HIIT remain to be determined. Furthermore, the specific features of an ideal HIIT program (i.e., exercise intensity, duration of each interval bout, rest intervals between bouts, number of interval bouts per session and number of HIIT sessions per week) have yet to be fully evaluated (Garber et al., 2011). Given these considerations, a conservative approach to HIIT is recommended [e.g., three, 5 x 5-minute interval bouts at 85−95% HRR or VO2R, with five minutes of active recovery at an intensity below 40% HRR or VO2R, on one or two days per week (Gormley et al., 2008)].
From Theory to Practice
In summary, key training considerations for the enhancement of cardiorespiratory fitness include exceeding the minimal training threshold intensity, weekly volume of exercise and judicious use of HIIT. Clearly, given that low cardiorespiratory fitness accounts for more deaths in both men and women than any other CVD risk factor, clients should be strongly encouraged to list improved cardiorespiratory fitness as one of their primary program goals.
References
American College of Sports Medicine (2010). ACSM’s Guidelines for Exercise Testing and Prescription (8th ed.). Baltimore, Md.: Wolters Kluwer/Lippincott Williams & Wilkins.
Blair, S.N. (2009). Physical inactivity: The biggest public health problem of the 21st century. British Journal of Sports Medicine, 43, 1−2.
Blair, S.N. et al. (1996). Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women. Journal of the American Medical Association, 276, 205−210.
Blair, S.N. et al. (1989). Physical fitness and all-cause mortality: A prospective study of healthy men and women. Journal of the American Medical Association, 262, 2395−2401.
Church, T.S. et al. (2007). Effects of different doses of physical activity on cardiorespiratory fitness among sedentary, overweight or obese postmenopausal women with elevated blood pressure: A randomized controlled trial. Journal of the American Medical Association, 297, 2081−2091.
Church, T.S. et al. (2005). Cardiorespiratory fitness and body mass index as predictors of cardiovascular disease mortality among men with diabetes. Archives of Internal Medicine, 165, 2114−2120.
Costill, D.L. (1970). Metabolic responses during distance running. Journal of Applied Physiology, 28, 96−100.
Franklin, B.A. (2007). Fitness: The ultimate marker for risk stratification and health outcomes? Preventive Cardiology, 10, 42–6.
Garber, C.E. et al. (2011). Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Medicine & Science in Sports & Exercise, 43, 1334−1359.
Gill, J.M.R. and Malkova, D. (2006). Physical activity, fitness and cardiovascular disease risk in adults: Interactions with insulin resistance and obesity. Clinical Science, 110, 409−425.
Gormley, S.E. et al. (2008). Effect of intensity of aerobic training on VO2max. Medicine & Science in Sports & Exercise, 40, 1336–1343.
Horowitz, J.F. (2007). Exercise-induced alterations in muscle lipid metabolism improves insulin sensitivity. Exercise and Sports Sciences Review, 35, 192−196.
Swain, D.P. and Franklin, B.A. (2002). VO2 reserve and the minimal intensity for improving cardiorespiratory fitness. Medicine & Science in Sports & Exercise, 34, 152−157.
Williams, P.T. (2001). Physical fitness and activity as separate heart disease risk factors: A meta-analysis. Medicine & Science in Sports & Exercise, 33, 754−761.
________________________________________________________________________

Lance C. Dalleck, Ph.D., is academic coordinator of the cardiac rehabilitation postgraduate program at the University of Auckland in New Zealand. His research interests include improving exercise performance and health outcomes through evidence-based practice, quantifying the energy expenditure of outdoor and non-traditional types of physical activity, and studying historical perspectives in health, fitness and exercise physiology.